南方医科大学学报 ›› 2026, Vol. 46 ›› Issue (2): 394-402.doi: 10.12122/j.issn.1673-4254.2026.02.17
• • 上一篇
余晖豪1( ), 邵玉2, 程倩倩3, 周新瑞1, 耿海萍1, 杨燕1()
), 邵玉2, 程倩倩3, 周新瑞1, 耿海萍1, 杨燕1()
收稿日期:2025-05-29
出版日期:2026-02-20
发布日期:2026-03-10
通讯作者:
杨燕
E-mail:yuhh0602@163.com;qiannianhupo@163.com
作者简介:余晖豪,在读硕士研究生,E-mail: yuhh0602@163.com
基金资助:
Huihao YU1(), Yu SHAO2, Qianqian CHENG3, Xinrui ZHOU1, Haiping GENG1, Yan YANG1()
Received:2025-05-29
Online:2026-02-20
Published:2026-03-10
Contact:
Yan YANG
E-mail:yuhh0602@163.com;qiannianhupo@163.com
摘要:
目的 明确膜棕榈酰化蛋白6(MPP6)在肝细胞癌(HCC)中的表达,分析其表达与HCC患者临床病理特征和预后的关系,探讨其对HCC细胞生物学行为的影响。 方法 选取2017年1月~2019年12月在我院行手术治疗的118例HCC患者肿瘤及癌旁组织标本,收集患者的临床病理资料,随访患者总生存期。采用免疫组化分析MPP6在肿瘤和癌旁组织中的表达水平;采用Cox回归分析MPP6表达水平与HCC患者临床病理特征和患者总生存期的相关性;采用平板克隆、划痕实验、Transwell实验和流式细胞术检测MPP6对HCC细胞Hep3B生物学行为的影响。 结果 与癌旁组织相比,MPP6在HCC组织中高表达(P<0.001);MPP6表达水平与患者肝硬化背景(P=0.028)和基线白蛋白水平(P=0.035)相关;生存分析提示,高表达MPP6患者预后较差(P<0.001);Cox回归分析显示,MPP6表达水平是患者总生存期的独立预测因素(P=0.012,HR:2.335,95% CI: 1.502~3.629)。体外敲减MPP6可致Hep3B细胞增殖、迁移及侵袭能力下降(P<0.05),并阻滞细胞周期于G0/G1期(P<0.001)。 结论 MPP6在HCC组织中高表达,并与HCC患者重要临床病理特征、不良预后相关;体外敲减MPP6可抑制HCC细胞增殖、迁移和侵袭能力并阻滞细胞周期于G0/G1期。
余晖豪, 邵玉, 程倩倩, 周新瑞, 耿海萍, 杨燕. 肝细胞癌中MPP6高表达预测患者不良预后并促进肿瘤恶性生物学行为[J]. 南方医科大学学报, 2026, 46(2): 394-402.
Huihao YU, Yu SHAO, Qianqian CHENG, Xinrui ZHOU, Haiping GENG, Yan YANG. High expression of MPP6 predicts poor patient prognosis and promotes malignant biological behaviors of hepatocellular carcinoma cells[J]. Journal of Southern Medical University, 2026, 46(2): 394-402.
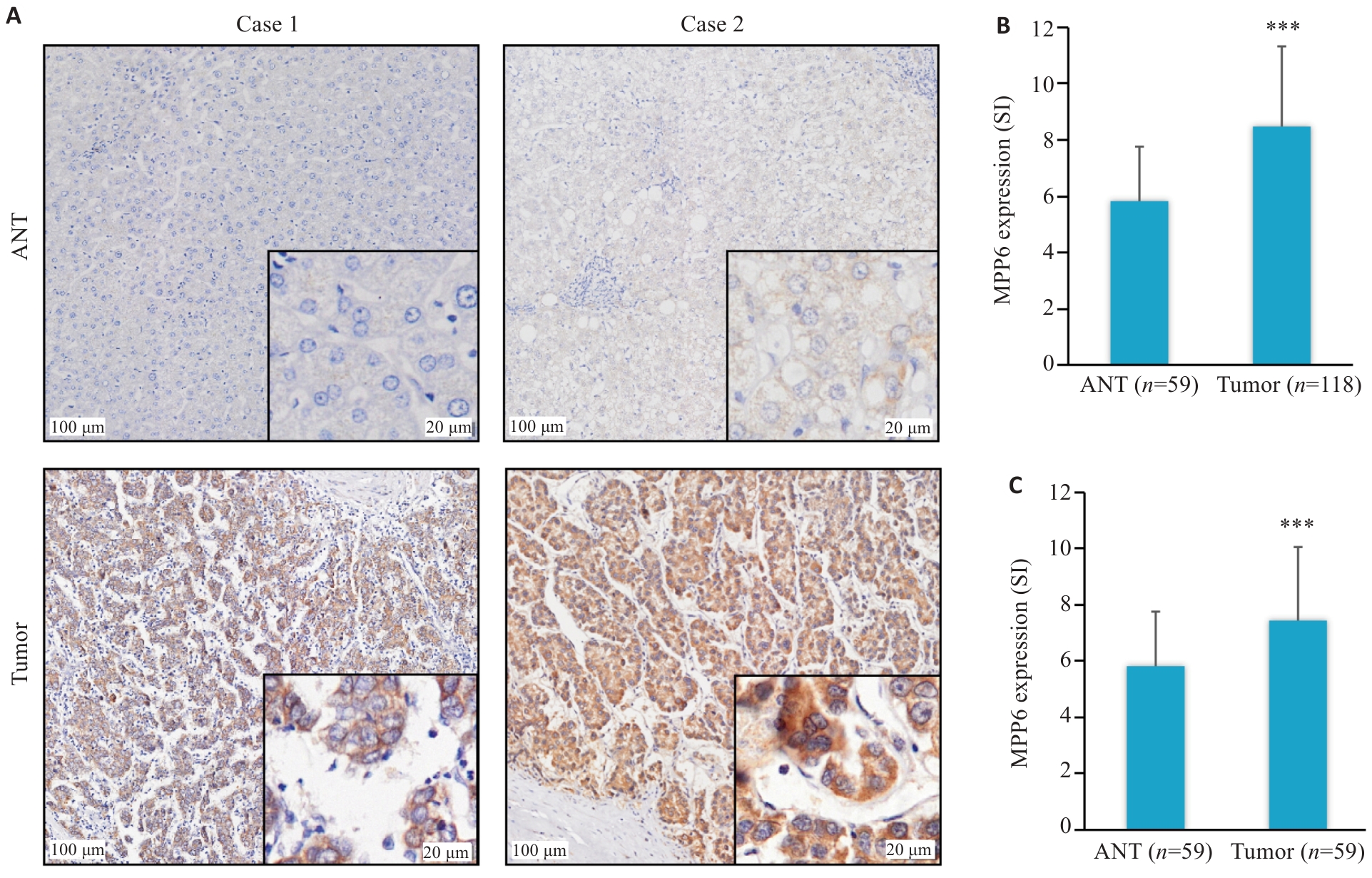
图1 MPP6在HCC组织中的表达情况
Fig.1 Expression of MPP6 in HCC tissues. A: Representative images of differential expression of MPP6 in HCC and ANT tissues. B: Differential expressions of MPP6 in 118 HCC tissues and 59 ANT tissues. C: Differential expressions of MPP6 in 59 pairs of HCC and ANT tissues. ***P<0.001 vs ANT.
| Factor | n | Low MPP6 expression | High MPP6 expression | P |
|---|---|---|---|---|
| Age (year) | ||||
| ≤60 | 75 | 29 (38.7%) | 46 (61.3%) | 0.557 |
| >60 | 43 | 19 (44.2%) | 24 (55.8%) | |
| Gender | ||||
| Female | 24 | 12 (50.0%) | 12 (50.0%) | 0.298 |
| Male | 94 | 36 (38.3%) | 58 (61.7%) | |
| Hepatic sclerosis | ||||
| No | 23 | 14 (60.9%) | 9 (39.1%) | 0.028 |
| Yes | 95 | 34 (35.8%) | 61 (64.2%) | |
| Child-Pugh | ||||
| A | 109 | 42 (38.5%) | 67 (61.5%) | 0.156 |
| B | 9 | 6 (66.7%) | 3 (33.3%) | |
| Alpha-fetoprotei (ng/mL)# | ||||
| ≤20 | 53 | 19 (35.8%) | 34 (64.2%) | 0.348 |
| >20 | 63 | 28 (44.4%) | 35 (55.6%) | |
| Alanine aminotransferase (U/L) | ||||
| ≤45 | 92 | 35 (38.0%) | 57 (62.0%) | 0.273 |
| >45 | 26 | 13 (50.0%) | 13 (50.0%) | |
| Glutamyltransferase (U/L) | ||||
| ≤45 | 61 | 28 (45.9%) | 33 (54.1%) | 0.232 |
| >45 | 57 | 20 (35.1%) | 37 (64.9%) | |
| Albumin (mg/L) | ||||
| ≤40 | 55 | 28 (50.9%) | 27 (49.1%) | 0.035 |
| >40 | 63 | 20 (31.7%) | 43 (68.3%) | |
| Tumor size (cm) | ||||
| ≤5 | 65 | 29 (44.6%) | 36 (55.4%) | 0.335 |
| >5 | 53 | 19 (35.8%) | 34 (64.2%) | |
| Tumor number | ||||
| Single | 98 | 40 (40.8%) | 58 (59.2%) | 0.628 |
| Multiple | 20 | 8 (40.0%) | 12 (60.0%) | |
| Tumor capsule | ||||
| Complete | 3 | 1 (33.3%) | 2 (66.7%) | 0.793 |
| Incomplete | 115 | 47 (40.9%) | 68 (59.1%) | |
| Portal vein branch tumor thrombus | ||||
| Yes | 5 | 1 (20.0%) | 4 (80.0%) | 0.336 |
| No | 113 | 47 (41.6%) | 66 (58.4%) | |
| BCLC staging | ||||
| 0-A | 49 | 24 (49.0%) | 25 (51.0%) | 0.127 |
| B-C | 69 | 23 (33.3%) | 46 (66.7%) |
表1 MPP6表达与HCC患者临床病理特征的相关性分析
Tab.1 Correlation analysis between MPP6 expression and clinicopathological features of HCC patients
| Factor | n | Low MPP6 expression | High MPP6 expression | P |
|---|---|---|---|---|
| Age (year) | ||||
| ≤60 | 75 | 29 (38.7%) | 46 (61.3%) | 0.557 |
| >60 | 43 | 19 (44.2%) | 24 (55.8%) | |
| Gender | ||||
| Female | 24 | 12 (50.0%) | 12 (50.0%) | 0.298 |
| Male | 94 | 36 (38.3%) | 58 (61.7%) | |
| Hepatic sclerosis | ||||
| No | 23 | 14 (60.9%) | 9 (39.1%) | 0.028 |
| Yes | 95 | 34 (35.8%) | 61 (64.2%) | |
| Child-Pugh | ||||
| A | 109 | 42 (38.5%) | 67 (61.5%) | 0.156 |
| B | 9 | 6 (66.7%) | 3 (33.3%) | |
| Alpha-fetoprotei (ng/mL)# | ||||
| ≤20 | 53 | 19 (35.8%) | 34 (64.2%) | 0.348 |
| >20 | 63 | 28 (44.4%) | 35 (55.6%) | |
| Alanine aminotransferase (U/L) | ||||
| ≤45 | 92 | 35 (38.0%) | 57 (62.0%) | 0.273 |
| >45 | 26 | 13 (50.0%) | 13 (50.0%) | |
| Glutamyltransferase (U/L) | ||||
| ≤45 | 61 | 28 (45.9%) | 33 (54.1%) | 0.232 |
| >45 | 57 | 20 (35.1%) | 37 (64.9%) | |
| Albumin (mg/L) | ||||
| ≤40 | 55 | 28 (50.9%) | 27 (49.1%) | 0.035 |
| >40 | 63 | 20 (31.7%) | 43 (68.3%) | |
| Tumor size (cm) | ||||
| ≤5 | 65 | 29 (44.6%) | 36 (55.4%) | 0.335 |
| >5 | 53 | 19 (35.8%) | 34 (64.2%) | |
| Tumor number | ||||
| Single | 98 | 40 (40.8%) | 58 (59.2%) | 0.628 |
| Multiple | 20 | 8 (40.0%) | 12 (60.0%) | |
| Tumor capsule | ||||
| Complete | 3 | 1 (33.3%) | 2 (66.7%) | 0.793 |
| Incomplete | 115 | 47 (40.9%) | 68 (59.1%) | |
| Portal vein branch tumor thrombus | ||||
| Yes | 5 | 1 (20.0%) | 4 (80.0%) | 0.336 |
| No | 113 | 47 (41.6%) | 66 (58.4%) | |
| BCLC staging | ||||
| 0-A | 49 | 24 (49.0%) | 25 (51.0%) | 0.127 |
| B-C | 69 | 23 (33.3%) | 46 (66.7%) |
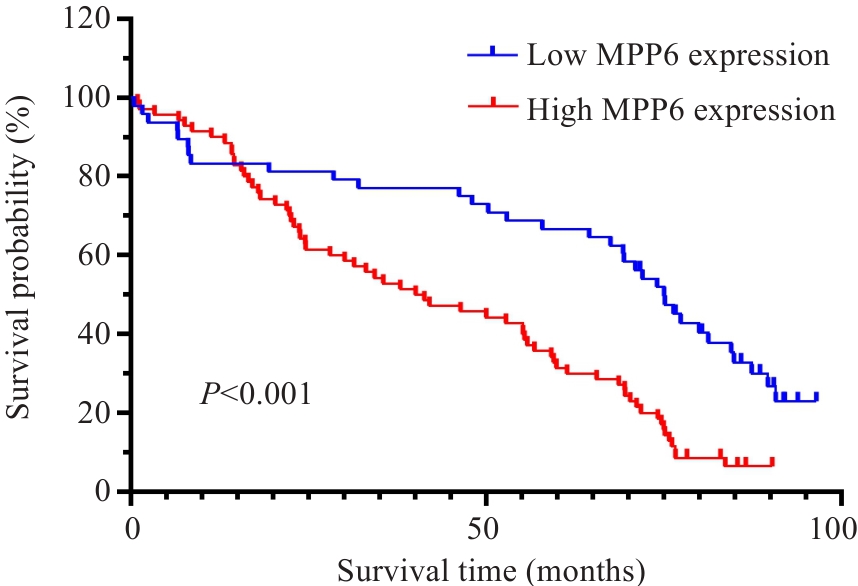
图2 MPP6不同表达水平下HCC患者的OS生存曲线
Fig.2 Survival curve for overall survival (OS) of HCC patients with low and high MPP6 expression levels.
| Factor | n | HR | 95%CI | P |
|---|---|---|---|---|
| Age (year) | ||||
| ≤60 | 75 | 1.404 | 0.932-2.114 | 0.105 |
| >60 | 43 | |||
| Gender | ||||
| Female | 24 | 1.027 | 0.621-1.697 | 0.919 |
| Male | 94 | |||
| Hepatic sclerosis | ||||
| No | 23 | 0.769 | 0.471-1.257 | 0.295 |
| Yes | 95 | |||
| Child-Pugh | ||||
| A | 109 | 0.925 | 0.448-1.912 | 0.834 |
| B | 9 | |||
| Alpha-fetoprotei (ng/mL)# | ||||
| ≤20 | 53 | 0.746 | 0.500-1.113 | 0.151 |
| >20 | 63 | |||
| Alanine aminotransferase (U/L) | ||||
| ≤45 | 92 | 1.441 | 0.909-2.287 | 0.120 |
| >45 | 26 | |||
| Glutamyltransferase (U/L) | ||||
| ≤45 | 61 | 1.464 | 0.983-2.180 | 0.061 |
| >45 | 57 | |||
| Albumin (mg/L) | ||||
| ≤40 | 55 | 1.064 | 0.712-1.591 | 0.761 |
| >40 | 63 | |||
| Tumor size (cm) | ||||
| ≤5 | 65 | 1.578 | 1.062-2.346 | 0.024 |
| >5 | 53 | |||
| Tumor number | ||||
| Single | 98 | 1.297 | 0.786-2.140 | 0.309 |
| Multiple | 20 | |||
| Tumor capsule | ||||
| Complete | 3 | 2.083 | 0.655-6.623 | 0.214 |
| Incomplete | 115 | |||
| Portal vein branch tumor thrombus | ||||
| Yes | 5 | 2.437 | 0.985-6.028 | 0.054 |
| No | 113 | |||
| BCLC staging | ||||
| 0-A | 49 | 1.497 | 0.995-2.251 | 0.053 |
| B-C | 64 | |||
| Postoperative treatment | ||||
| No | 42 | 0.771 | 0.511-1.612 | 0.214 |
| Yes | 76 | |||
| MPP6 Expression | ||||
| Low | 48 | 2.450 | 1.584-3.788 | <0.001 |
| High | 70 |
表2 HCC术后患者OS预后因素的单因素Cox回归分析
Tab.2 Univariate Cox regression analysis of prognostic factors for OS in postoperative HCC patients
| Factor | n | HR | 95%CI | P |
|---|---|---|---|---|
| Age (year) | ||||
| ≤60 | 75 | 1.404 | 0.932-2.114 | 0.105 |
| >60 | 43 | |||
| Gender | ||||
| Female | 24 | 1.027 | 0.621-1.697 | 0.919 |
| Male | 94 | |||
| Hepatic sclerosis | ||||
| No | 23 | 0.769 | 0.471-1.257 | 0.295 |
| Yes | 95 | |||
| Child-Pugh | ||||
| A | 109 | 0.925 | 0.448-1.912 | 0.834 |
| B | 9 | |||
| Alpha-fetoprotei (ng/mL)# | ||||
| ≤20 | 53 | 0.746 | 0.500-1.113 | 0.151 |
| >20 | 63 | |||
| Alanine aminotransferase (U/L) | ||||
| ≤45 | 92 | 1.441 | 0.909-2.287 | 0.120 |
| >45 | 26 | |||
| Glutamyltransferase (U/L) | ||||
| ≤45 | 61 | 1.464 | 0.983-2.180 | 0.061 |
| >45 | 57 | |||
| Albumin (mg/L) | ||||
| ≤40 | 55 | 1.064 | 0.712-1.591 | 0.761 |
| >40 | 63 | |||
| Tumor size (cm) | ||||
| ≤5 | 65 | 1.578 | 1.062-2.346 | 0.024 |
| >5 | 53 | |||
| Tumor number | ||||
| Single | 98 | 1.297 | 0.786-2.140 | 0.309 |
| Multiple | 20 | |||
| Tumor capsule | ||||
| Complete | 3 | 2.083 | 0.655-6.623 | 0.214 |
| Incomplete | 115 | |||
| Portal vein branch tumor thrombus | ||||
| Yes | 5 | 2.437 | 0.985-6.028 | 0.054 |
| No | 113 | |||
| BCLC staging | ||||
| 0-A | 49 | 1.497 | 0.995-2.251 | 0.053 |
| B-C | 64 | |||
| Postoperative treatment | ||||
| No | 42 | 0.771 | 0.511-1.612 | 0.214 |
| Yes | 76 | |||
| MPP6 Expression | ||||
| Low | 48 | 2.450 | 1.584-3.788 | <0.001 |
| High | 70 |
| Factor | n | HR | 95% CI | P |
|---|---|---|---|---|
| Tumor size (cm) | ||||
| ≤5 | 65 | 1.405 | 0.941-2.098 | 0.096 |
| >5 | 53 | |||
| MPP6 Expression | ||||
| Low | 48 | 2.335 | 1.502-3.629 | 0.012 |
| High | 70 |
表3 HCC术后患者OS预后因素的多因素Cox回归分析
Tab.3 Multivariate Cox regression analysis of prognostic factors for OS in postoperative HCC patients
| Factor | n | HR | 95% CI | P |
|---|---|---|---|---|
| Tumor size (cm) | ||||
| ≤5 | 65 | 1.405 | 0.941-2.098 | 0.096 |
| >5 | 53 | |||
| MPP6 Expression | ||||
| Low | 48 | 2.335 | 1.502-3.629 | 0.012 |
| High | 70 |
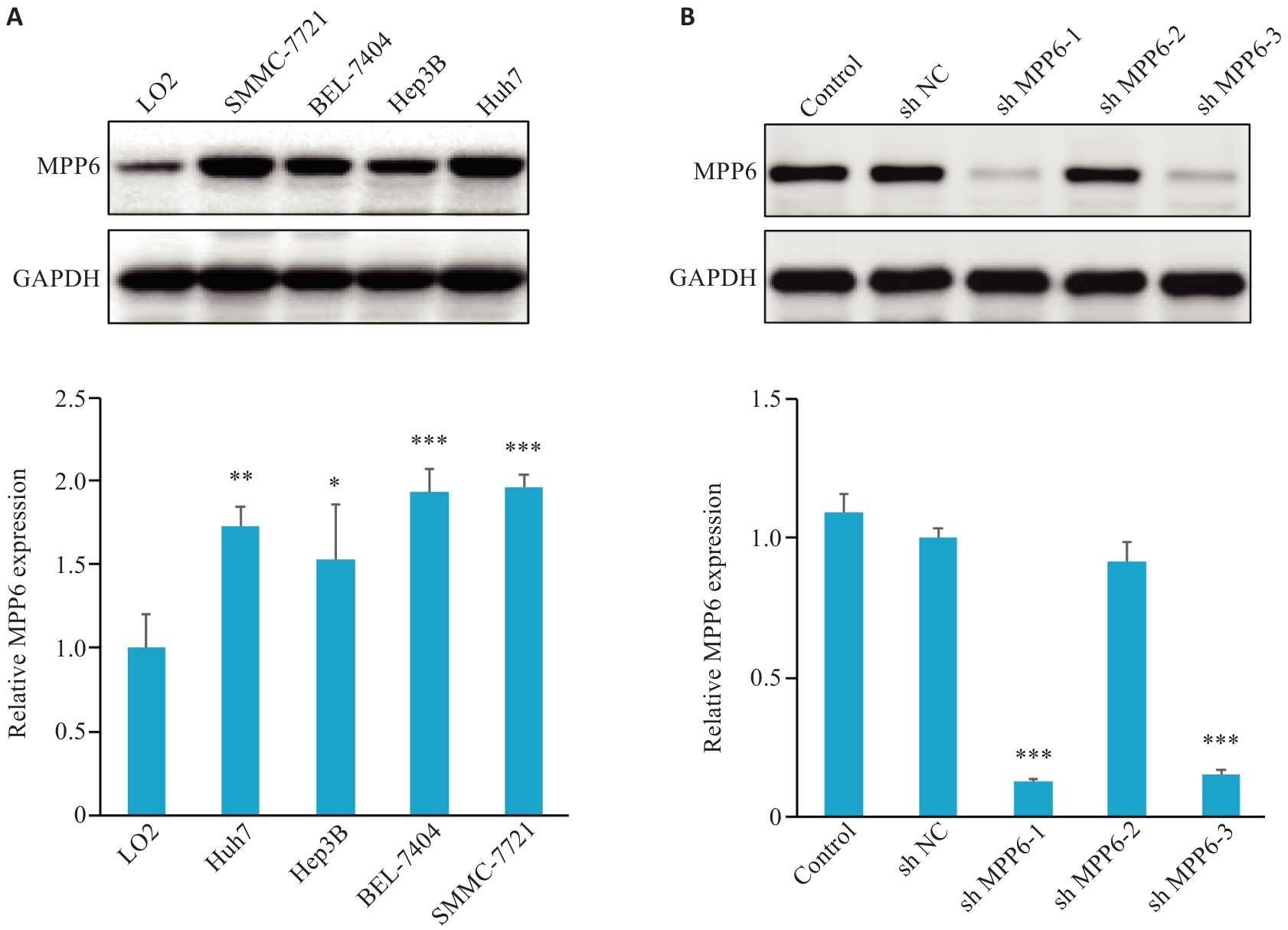
图3 敲减MPP6基因的Hep3B细胞筛选与构建
Fig.3 HCC cell screening and construction of Hep3B cells with MPP6 gene knockdown. A: Western blotting for detecting expression level of MPP6 in different HCC cell lines (*P<0.05, **P<0.01, ***P<0.001 vs LO2 cells). B: Western blotting for assessing efficiency of MPP6 gene knockdown in Hep3B cells (***P<0.001 vs sh NC).
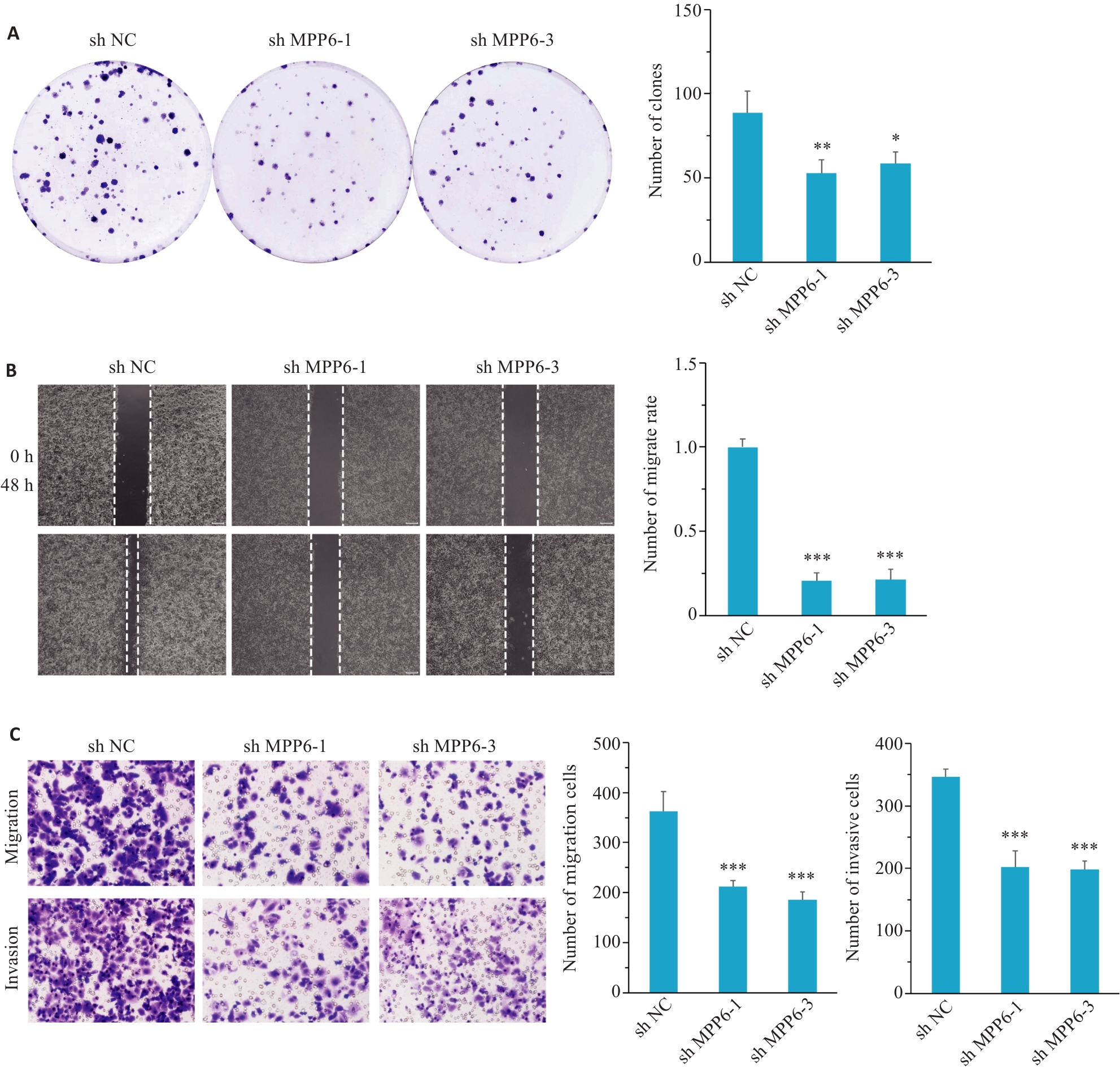
图4 敲减MPP6基因对Hep3B细胞增殖、迁移和侵袭的影响
Fig.4 Effect of MPP6 knockdown on proliferation, migration and invasion of Hep3B cells. A: Colony formation assay for assessing cell proliferation following MPP6 knockdown. B: Wound-healing assay for assessing migration ability of Hep3B cells with MPP6 knockdown (Original magnification: ×40). C: Transwell assay for assessing migration and invasion capabilities of Hep3B cells with MPP6 knockdown (×100). *P<0.05, **P<0.01, ***P<0.001 vs sh NC.
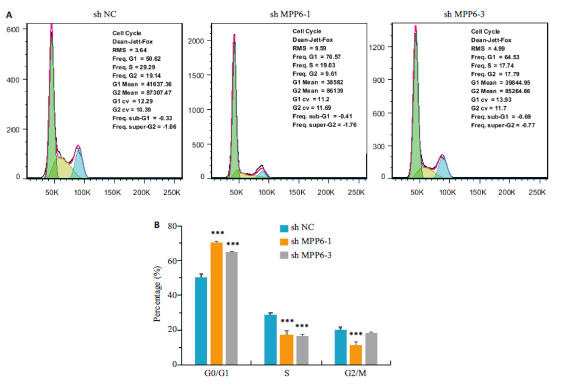
图5 敲减MPP6基因对Hep3B细胞周期分布的影响
Fig.5 Effect of MPP6 knockdown on cell cycle distribution of Hep3B cells. A: Flow cytometry for assessing the impact ofMPP6 knockdown on cell cycle distribution of Hep3B cells. B: Quantitative analysis of cell cycle distribution in Hep3Bcells. ***P<0.001 vs sh NC.
| [1] | Han BF, Zheng RS, Zeng HM, et al. Cancer incidence and mortality in China, 2022[J]. J Natl Cancer Cent, 2024, 4(1): 47-53. doi:10.1016/j.jncc.2024.01.006 |
| [2] | Jiang YB, Dong XF, Zhang YY, et al. Navigating the complexities: challenges and opportunities in conversion therapy for advanced hepatocellular carcinoma[J]. Clin Exp Med, 2025, 25(1): 169. doi:10.1007/s10238-025-01698-9 |
| [3] | Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma[J]. Nat Rev Dis Primers, 2021, 7: 6. doi:10.1038/s41572-020-00240-3 |
| [4] | 张力苹, 刘喜娟, 胡 潇, 等. 经动脉化疗栓塞续贯肝动脉灌注化疗联合TKI和PD-1单抗在晚期肝癌一线治疗中的疗效观察[J]. 南方医科大学学报, 2024, 44(9):1831-8. doi:10.12122/j.issn.1673-4254.2024.09.24 |
| [5] | Wang Y, Deng BC. Hepatocellular carcinoma: molecular mechanism, targeted therapy, and biomarkers[J]. Cancer Metastasis Rev, 2023, 42(3): 629-52. doi:10.1007/s10555-023-10084-4 |
| [6] | Cen CH, Liu XY, He W, et al. Novel approaches in CRISPR/Cas12a-based sensing for HCC diagnosis - A review (2020–2025)[J]. J Pharm Biomed Anal, 2025, 262: 116878. doi:10.1016/j.jpba.2025.116878 |
| [7] | 南月敏, 赵素贤, 刘领弟. 肝细胞癌早诊早治技术研究进展与临床应用[J]. 中华肝脏病杂志, 2025, 33(4):307-9. |
| [8] | Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023[J]. CA A Cancer J Clinicians, 2023, 73(1): 17-48. doi:10.3322/caac.21763 |
| [9] | Liu QY, Wang JH, Guo ZX, et al. CMTM6 promotes hepatocellular carcinoma progression through stabilizing β-catenin[J]. Cancer Lett, 2024, 583: 216585. doi:10.1016/j.canlet.2023.216585 |
| [10] | Chytła A, Gajdzik-Nowak W, Olszewska P, et al. Not just another scaffolding protein family: the multifaceted MPPs[J]. Molecules, 2020, 25(21): E4954. doi:10.3390/molecules25214954 |
| [11] | Schilders G, Raijmakers R, Raats JM, et al. MPP6 is an exosome-associated RNA-binding protein involved in 5.8S rRNA maturation[J]. Nucleic Acids Res, 2005, 33(21): 6795-804. doi:10.1093/nar/gki982 |
| [12] | Xu F, Si X, Du J, et al. Downregulating SynCAM and MPP6 expression is associated with ovarian cancer progression[J]. Oncol Lett, 2019, 18(3): 2477-83. |
| [13] | Djurec M, Graña O, Lee A, et al. Saa3 is a key mediator of the protumorigenic properties of cancer-associated fibroblasts in pancreatic tumors[J]. Proc Natl Acad Sci USA, 2018, 115(6): E1147-56. doi:10.1073/pnas.1717802115 |
| [14] | Cheng Q, Wang W, Liu J, et al. Elevated MPP6 expression correlates with an unfavorable prognosis, angiogenesis and immune evasion in hepatocellular carcinoma[J]. Front Immunol, 2023, 14: 1173848. doi:10.3389/fimmu.2023.1173848 |
| [15] | 中华人民共和国国家卫生健康委员会医政司. 原发性肝癌诊疗指南(2024年版)[J]. 协和医学杂志, 2024, 15(3):532-59. |
| [16] | Song J, Liu Y, Liu F, et al. The 14-3-3σ protein promotes HCC anoikis resistance by inhibiting EGFR degradation and thereby activating the EGFR-dependent ERK1/2 signaling pathway[J]. Theranostics, 2021, 11(3): 996-1015. doi:10.7150/thno.51646 |
| [17] | Mabeta P, Steenkamp V. The VEGF/VEGFR axis revisited: implications for cancer therapy[J]. Int J Mol Sci, 2022, 23(24): 15585. doi:10.3390/ijms232415585 |
| [18] | Xiang Z, Li JR, Xu YY, et al. Cell differentiation-related signaling pathways in hepatocellular carcinoma metastasis[J]. Cancer Lett, 2025, 627: 217846. doi:10.1016/j.canlet.2025.217846 |
| [19] | Chastney MR, Kaivola J, Leppänen VM, et al. The role and regulation of integrins in cell migration and invasion[J]. Nat Rev Mol Cell Biol, 2025, 26(2): 147-67. doi:10.1038/s41580-024-00777-1 |
| [20] | Li Y, Liu F, Cai Q, et al. Invasion and metastasis in cancer: molecular insights and therapeutic targets[J]. Signal Transduct Target Ther, 2025, 10(1): 57. doi:10.1038/s41392-025-02148-4 |
| [21] | Zhang Y, Tang XL, Liu L, et al. GLO1 regulates hepatocellular carcinoma proliferation and migration through the cell cycle pathway[J]. BMC Cancer, 2024, 24(1): 1297. doi:10.1186/s12885-024-12927-x |
| [22] | Nair G, Saraswathy GR, Aranjani JM, et al. Unraveling a novel therapeutic facet of Etravirine to confront Hepatocellular Carcinoma via disruption of cell cycle[J]. Sci Rep, 2025, 15(1): 4979. doi:10.1038/s41598-025-87676-3 |
| [23] | 张 诺, 张 震, 张雨路, 等. PCID2在胃癌组织中高表达并通过调控细胞周期进程和增殖影响患者预后[J]. 南方医科大学学报, 2024, 44(2):324-32. |
| [24] | Gaillard H, García-Muse T, Aguilera A. Replication stress and cancer[J]. Nat Rev Cancer, 2015, 15(5): 276-89. doi:10.1038/nrc3916 |
| [25] | Hanahan D. Hallmarks of cancer: new dimensions[J]. Cancer Discov, 2022, 12(1): 31-46. doi:10.1158/2159-8290.cd-21-1059 |
| [26] | Yang Y, Zhang N, Zhu J, et al. Downregulated connexin32 promotes EMT through the Wnt/β-catenin pathway by targeting Snail expression in hepatocellular carcinoma[J]. Int J Oncol, 2017, 50(6): 1977-88. doi:10.3892/ijo.2017.3985 |
| [27] | Tang L, Ji Y, Ni C, et al. EIF4A3-mediated biogenesis of CircFADS1 promotes the progression of hepatocellular carcinoma via Wnt/β-catenin pathway[J]. Adv Sci: Weinh, 2025, 12(14): e2411869. doi:10.1002/advs.202411869 |
| [28] | Wang JH, Yu HM, Dong W, et al. N6-methyladenosine–mediated up-regulation of FZD10 regulates liver cancer stem cells’ properties and lenvatinib resistance through WNT/β-catenin and hippo signaling pathways[J]. Gastroenterology, 2023, 164(6): 990-1005. doi:10.1053/j.gastro.2023.01.041 |
| [1] | 梁笑笑, 栾慧林, 马鹏珍, 邓文珠, 金佳欣, 全晨阳, 陈婷婷, 杨友财, 谢颖桢. 基于生命八要素的心血管健康评分与缺血性脑卒中预后相关性及临床检验指标的中介效应:一项多中心前瞻性队列研究[J]. 南方医科大学学报, 2026, 46(2): 239-246. |
| [2] | 赵新丽, 王豪杰, 宋银春, 袁帅, 张振, 周星琦, 李姗姗, 李娴, 李锋. ERI3在肝癌中高表达并与患者不良预后相关[J]. 南方医科大学学报, 2026, 46(1): 175-182. |
| [3] | 沙桐, 王文研, 宣佳斌, 吴洁, 石能贤, 何劲, 胡鸿彬, 张耀元. 基于Th1/Th2细胞因子检测的脓毒症免疫状态分型及预后分析:一项回顾性研究[J]. 南方医科大学学报, 2026, 46(1): 6-22. |
| [4] | 王莹, 李静, 王伊迪, 华明钰, 胡玮彬, 张晓智. 原发性肝癌患者的临床结局与治疗反应预测模型:基于失巢凋亡和免疫基因[J]. 南方医科大学学报, 2025, 45(9): 1967-1979. |
| [5] | 张瑜, 李海涛, 潘玉卿, 曹杰贤, 翟丽, 张曦. MZB1基因在泛癌中的表达及其与免疫浸润及预后的关系[J]. 南方医科大学学报, 2025, 45(9): 2006-2018. |
| [6] | 王子良, 陈孝华, 杨晶晶, 严晨, 张志郅, 黄炳轶, 赵萌, 刘嵩, 葛思堂, 左芦根, 陈德利. 高表达SURF4通过抑制紧密连接蛋白表达促进胃癌细胞的恶性生物学行为[J]. 南方医科大学学报, 2025, 45(8): 1732-1742. |
| [7] | 庞金龙, 赵新丽, 张振, 王豪杰, 周星琦, 杨玉梅, 李姗姗, 常小强, 李锋, 李娴. 皮肤黑色素瘤中MMRN2高表达促进肿瘤细胞的侵袭和迁移并与不良预后相关[J]. 南方医科大学学报, 2025, 45(7): 1479-1489. |
| [8] | 吴璇, 方家敏, 韩玮玮, 陈琳, 孙菁, 金齐力. 高表达PRELID1促进胃癌细胞上皮间质转化并与不良预后相关[J]. 南方医科大学学报, 2025, 45(7): 1535-1542. |
| [9] | 王康, 李海宾, 余靖, 孟源, 张虹丽. ELFN1高表达是结肠癌的预后生物标志物并促进结肠癌细胞的增殖转移[J]. 南方医科大学学报, 2025, 45(7): 1543-1553. |
| [10] | 张毅, 沈昱, 万志强, 陶嵩, 柳亚魁, 王栓虎. CDKN3高表达促进胃癌细胞的迁移和侵袭:基于调控p53/NF-κB信号通路和抑制胃癌细胞凋亡[J]. 南方医科大学学报, 2025, 45(4): 853-861. |
| [11] | 黄晴晴, 张文静, 张小凤, 王炼, 宋雪, 耿志军, 左芦根, 王月月, 李静, 胡建国. 高表达MYO1B促进胃癌细胞增殖、迁移和侵袭并与患者的不良预后有关[J]. 南方医科大学学报, 2025, 45(3): 622-631. |
| [12] | 李华莉, 宋婷, 刘嘉雯, 李永宝, 姜兆静, 窦文, 周凌宏. 预后导向的肺癌调强放疗计划优化新方法[J]. 南方医科大学学报, 2025, 45(3): 643-649. |
| [13] | 宋雪, 陈悦, 张敏, 张诺, 左芦根, 李静, 耿志军, 张小凤, 王月月, 王炼, 胡建国. GPSM2在胃癌组织中高表达并通过促进肿瘤细胞的增殖影响患者预后[J]. 南方医科大学学报, 2025, 45(2): 229-238. |
| [14] | 唐天威, 李路安, 陈源汉, 张丽, 徐丽霞, 李志莲, 冯仲林, 张辉林, 华瑞芳, 叶智明, 梁馨苓, 李锐钊. 高血清胱抑素C水平是IgA肾病不良预后的独立危险因素[J]. 南方医科大学学报, 2025, 45(2): 379-386. |
| [15] | 李超, 殷国志, 程萧, 姜业臻. 血管相关迁移细胞蛋白在肝细胞癌中高表达并促进肝癌细胞侵袭转移[J]. 南方医科大学学报, 2025, 45(12): 2628-2638. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||