南方医科大学学报 ›› 2025, Vol. 45 ›› Issue (10): 2182-2190.doi: 10.12122/j.issn.1673-4254.2025.10.14
• • 上一篇
马会华1,2,3, 闫奎坡1,2( ), 刘刚1,2, 徐亚洲1,2, 张磊1,2, 李一卓1,2
), 刘刚1,2, 徐亚洲1,2, 张磊1,2, 李一卓1,2
收稿日期:2025-06-23
出版日期:2025-10-20
发布日期:2025-10-24
通讯作者:
闫奎坡
E-mail:ykp19821122@163.com
作者简介:马会华,在读硕士研究生,E-mail: 17790065627@163.com
基金资助:
Huihua MA1,2,3, Kuipo YAN1,2(), Gang LIU1,2, Yazhou XU1,2, Lei ZHANG1,2, Yizhuo LI1,2
Received:2025-06-23
Online:2025-10-20
Published:2025-10-24
Contact:
Kuipo YAN
E-mail:ykp19821122@163.com
摘要:
目的 分析1990~2021年中国和全球心房颤动/扑动(AF/AFL)疾病负担及其危险因素的变化情况,为我国AF/AFL制定有效的预防措施。 方法 基于GBD 2021数据库提供的1990~2021年204个国家或地区及全球的不同性别和不同年龄组中AF/AFL负担各项指数并进行标准化处理,使用joinpoint计算平均年百分比变化(AAPC)分析AF/AFL的趋势;此外,研究分析AF/AFL的发病率、患病率、死亡率和伤残调整寿命年(DALYs)来衡量AF/AFL的负担。最后分析AF/AFL的风险因素,并进一步采用孟德尔随机化分析验证其结果。 结果 1990~2021年,中国AF/AFL年龄标准化发病率(ASIR)从42.63/10万上升至44.93/10万,而全球呈下降趋势。中国AF/AFL年龄标准化死亡率(ASMR)从4.93/10万下降至4.33/10万,全球从4.24/10万上升到4.36/10万。中国AF/AFL年龄标准化DALY率(ASDR)从93.29/10万下降至93.29/10万,全球从100.81/10万增加至101.40/10万。中国及全球年龄和性别对AF/AFL负担影响存在显著差异(P<0.05)。男性ASIR与ASDR高于女性,但是女性ASMR与ASDR高于男性。中国AF/AFL发病率与患病率高于全球水平,但死亡率与DAYL率低于全球水平。在2021年,AF/AFL主要危险因素为高收缩压、高BMI、吸烟、酗酒、高钠饮食及低温等。除高收缩压外,吸烟是男性的重要因素,而女性主要则在于高体重指数的危险。 结论 中国AF/AFL发病与患病人数显著增加,人口基数大和老龄化问题成为重要公共卫生挑战;此外,居民应保持健康生活习惯,戒烟限酒,低钠饮食,定期筛查, 早发现早治疗。
马会华, 闫奎坡, 刘刚, 徐亚洲, 张磊, 李一卓. 1990~2021年心房颤动/扑动流行病学及其危险因素分析:基于2021年中国全球疾病负担研究与孟德尔随机化研究的系统分析[J]. 南方医科大学学报, 2025, 45(10): 2182-2190.
Huihua MA, Kuipo YAN, Gang LIU, Yazhou XU, Lei ZHANG, Yizhuo LI. Epidemiology of atrial fibrillation/atrial flutter and its risk factors from 1990 to 2021: a systematic analysis and Mendelian randomization study based on the China and Global Burden of Disease Study 2021[J]. Journal of Southern Medical University, 2025, 45(10): 2182-2190.
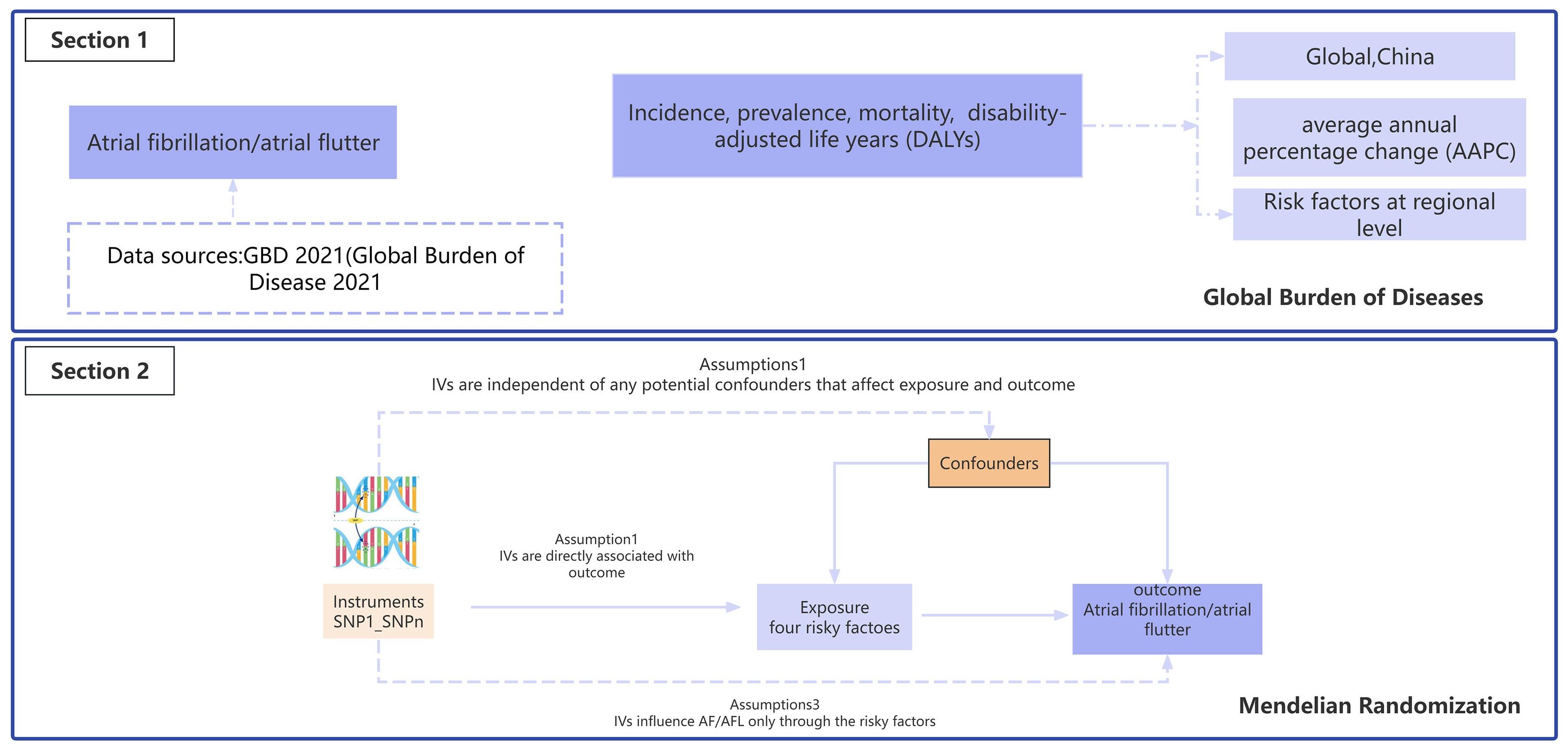
图1 研究设计流程图
Fig.1 Flowchart of the study design. Section 1: The Global Burden of Disease; Section 2: Assumptions and Mendelian randomization analysis in this study. Gene variants significantly associated with the variable factors phenotypes are used as the instrumental variables.
| Variable | Case | Data source | ID | Population |
|---|---|---|---|---|
| Exposure | European | |||
| Hypertension | 463 010 | MRC-IEU | ukb-b-12493 | European |
| BMI | 681 275 | GIANT | ieu-b-40 | European |
| Smoking | 607 291 | GSCAN | ieu-b-4877 | European |
| High alcohol | 112 117 | UK Biobank | ieu-a-1283 | European |
| Outcome | ||||
| AF/AFL | 463 010 | MRC-IEU | ukb-b-964 | European |
表1 MR数据来源
Tab.1 Summary of data source
| Variable | Case | Data source | ID | Population |
|---|---|---|---|---|
| Exposure | European | |||
| Hypertension | 463 010 | MRC-IEU | ukb-b-12493 | European |
| BMI | 681 275 | GIANT | ieu-b-40 | European |
| Smoking | 607 291 | GSCAN | ieu-b-4877 | European |
| High alcohol | 112 117 | UK Biobank | ieu-a-1283 | European |
| Outcome | ||||
| AF/AFL | 463 010 | MRC-IEU | ukb-b-964 | European |
| Location | Year | Incidence (10 000) | ASIR (/100 000) | Prevalence (10 000) | ASPR (/100 000) | Deaths (10 000) | ASMR (100 000) | DALYs (10 000) | ASDR (/100 000) |
|---|---|---|---|---|---|---|---|---|---|
| Total | |||||||||
| China | 1990 | 306 585 | 42.63 | 3 195 309 | 457.72 | 16 449 | 4.93 | 508 610 | 93.29 |
| 2021 | 916 180 | 44.92 | 10 775 721 | 524 | 64 728 | 4.33 | 1 653 117 | 89.76 | |
AAPC (%, 95% CI) | 0.16 (0.05-0.26) | 0.43 (0.32-0.54) | -0.45 (-0.78--0.1) | -0.12 (-0.32-0.07) | |||||
| Global | 1990 | 2 006 571 | 52.51 | 22 214 495 | 616.58 | 114 540 | 4.24 | 3 358 708 | 100.82 |
| 2021 | 4 484 926 | 52.12 | 52 552 045 | 620.51 | 338 947 | 4.36 | 8 358 894 | 101.40 | |
AAPC (%, 95% CI) | -0.02 (-0.05-0.00) | 0.02 (-0.02-0.06) | 0.11 (0.03-0.18) | 0.01 (-0.03-0.06) | |||||
| Male | |||||||||
| China | 1990 | 152 972 | 42 | 1 627 899 | 487.47 | 5207 | 3.56 | 221 887 | 81.96 |
| 2021 | 451 977 | 45.23 | 5 626 767 | 574.50 | 21 789 | 3.81 | 753 106 | 89.62 | |
AAPC (%, 95% CI) | 0.25 (0.10-0.4) | 0.52 (0.41-0.64) | 0.18 (-0.11-0.47) | 0.28 (0.09-0.46) | |||||
| Female | |||||||||
| China | 1990 | 153 613 | 41.74 | 1 567 410 | 429.293 | 11 242 | 5.54 | 286 723 | 97.72 |
| 2021 | 464 203 | 43.28 | 5 148 954 | 473.40 | 42 939 | 4.58 | 900 010 | 87.69 | |
AAPC (%, 95% CI) | 0.24 (0.10-0.2) | 0.27 (0.10-0.44) | -0.64 (-1.04--0.2) | -0.37 (-0.62--0.12) | |||||
| Male | |||||||||
| Global | 1990 | 1 015 287 | 57.99 | 11 492 470 | 727.79 | 42 677 | 4.20 | 1 569 927 | 109.93 |
| 2021 | 2 295 811 | 57.11 | 27 899 046 | 728.87 | 134 700 | 4.44 | 4 032 121 | 112.05 | |
AAPC (%, 95% CI) | -0.05 (-0.01--0.02) | -0.00 (-0.05-0.04) | 0.19 (0.09-0.30) | 0.06 (0.00-0.11) | |||||
| Female | |||||||||
| Global | 1990 | 991 284 | 47.43 | 10 722 025 | 529.53 | 71 862 | 4.25 | 1 788 781 | 93.29 |
| 2021 | 2 189 116 | 47.27 | 24 652 999 | 529.11 | 204 247 | 4.295 | 4 326 773 | 92.24 | |
AAPC (%, 95% CI) | -0.03 (-0.09-0.03) | -0.02 (-0.07-0.03) | 0.05 (-0.05-0.15) | -0.04 (-0.12- 0.04) |
表2 1990-2021年中国和全球心房颤动/扑动发病、患病、死亡、DALYs和相应的AAPC
Tab.2 Atrial fibrillation/atrial flutter incidence in China and globally from 1990 to 2021
| Location | Year | Incidence (10 000) | ASIR (/100 000) | Prevalence (10 000) | ASPR (/100 000) | Deaths (10 000) | ASMR (100 000) | DALYs (10 000) | ASDR (/100 000) |
|---|---|---|---|---|---|---|---|---|---|
| Total | |||||||||
| China | 1990 | 306 585 | 42.63 | 3 195 309 | 457.72 | 16 449 | 4.93 | 508 610 | 93.29 |
| 2021 | 916 180 | 44.92 | 10 775 721 | 524 | 64 728 | 4.33 | 1 653 117 | 89.76 | |
AAPC (%, 95% CI) | 0.16 (0.05-0.26) | 0.43 (0.32-0.54) | -0.45 (-0.78--0.1) | -0.12 (-0.32-0.07) | |||||
| Global | 1990 | 2 006 571 | 52.51 | 22 214 495 | 616.58 | 114 540 | 4.24 | 3 358 708 | 100.82 |
| 2021 | 4 484 926 | 52.12 | 52 552 045 | 620.51 | 338 947 | 4.36 | 8 358 894 | 101.40 | |
AAPC (%, 95% CI) | -0.02 (-0.05-0.00) | 0.02 (-0.02-0.06) | 0.11 (0.03-0.18) | 0.01 (-0.03-0.06) | |||||
| Male | |||||||||
| China | 1990 | 152 972 | 42 | 1 627 899 | 487.47 | 5207 | 3.56 | 221 887 | 81.96 |
| 2021 | 451 977 | 45.23 | 5 626 767 | 574.50 | 21 789 | 3.81 | 753 106 | 89.62 | |
AAPC (%, 95% CI) | 0.25 (0.10-0.4) | 0.52 (0.41-0.64) | 0.18 (-0.11-0.47) | 0.28 (0.09-0.46) | |||||
| Female | |||||||||
| China | 1990 | 153 613 | 41.74 | 1 567 410 | 429.293 | 11 242 | 5.54 | 286 723 | 97.72 |
| 2021 | 464 203 | 43.28 | 5 148 954 | 473.40 | 42 939 | 4.58 | 900 010 | 87.69 | |
AAPC (%, 95% CI) | 0.24 (0.10-0.2) | 0.27 (0.10-0.44) | -0.64 (-1.04--0.2) | -0.37 (-0.62--0.12) | |||||
| Male | |||||||||
| Global | 1990 | 1 015 287 | 57.99 | 11 492 470 | 727.79 | 42 677 | 4.20 | 1 569 927 | 109.93 |
| 2021 | 2 295 811 | 57.11 | 27 899 046 | 728.87 | 134 700 | 4.44 | 4 032 121 | 112.05 | |
AAPC (%, 95% CI) | -0.05 (-0.01--0.02) | -0.00 (-0.05-0.04) | 0.19 (0.09-0.30) | 0.06 (0.00-0.11) | |||||
| Female | |||||||||
| Global | 1990 | 991 284 | 47.43 | 10 722 025 | 529.53 | 71 862 | 4.25 | 1 788 781 | 93.29 |
| 2021 | 2 189 116 | 47.27 | 24 652 999 | 529.11 | 204 247 | 4.295 | 4 326 773 | 92.24 | |
AAPC (%, 95% CI) | -0.03 (-0.09-0.03) | -0.02 (-0.07-0.03) | 0.05 (-0.05-0.15) | -0.04 (-0.12- 0.04) |
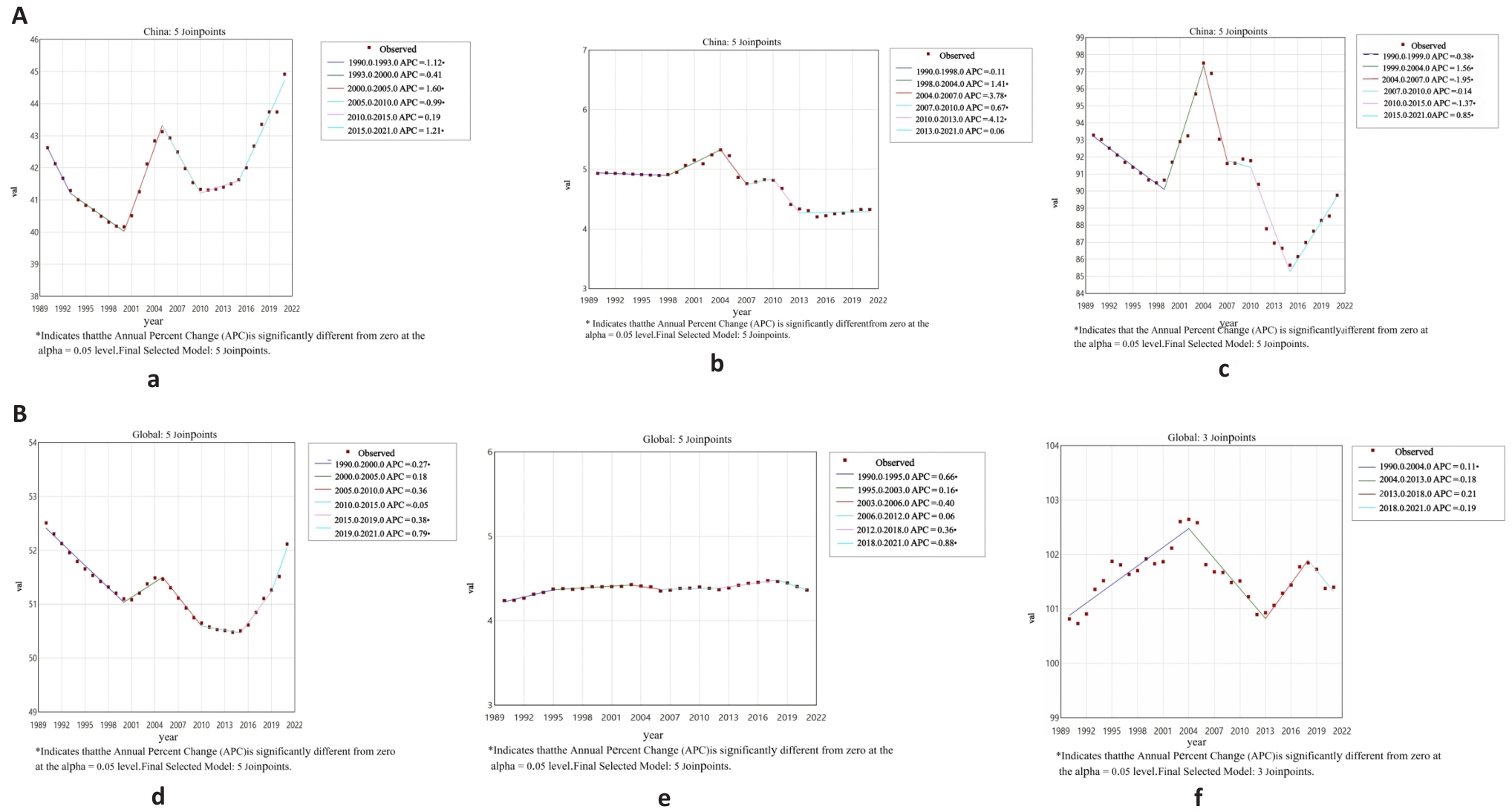
图2 1990~2021年中国和全球AF/AFL患者ASIR、ASPR、ASMR和ASDR的APC值
Fig.2 APC of ASIR, ASPR, ASMR, ASDR of AF/AFL in China and globally from 1990-2021. A: China. B: Global. a,d: ASIR; b, e: ASMR; c, f: ASDR, *P<0.05 .
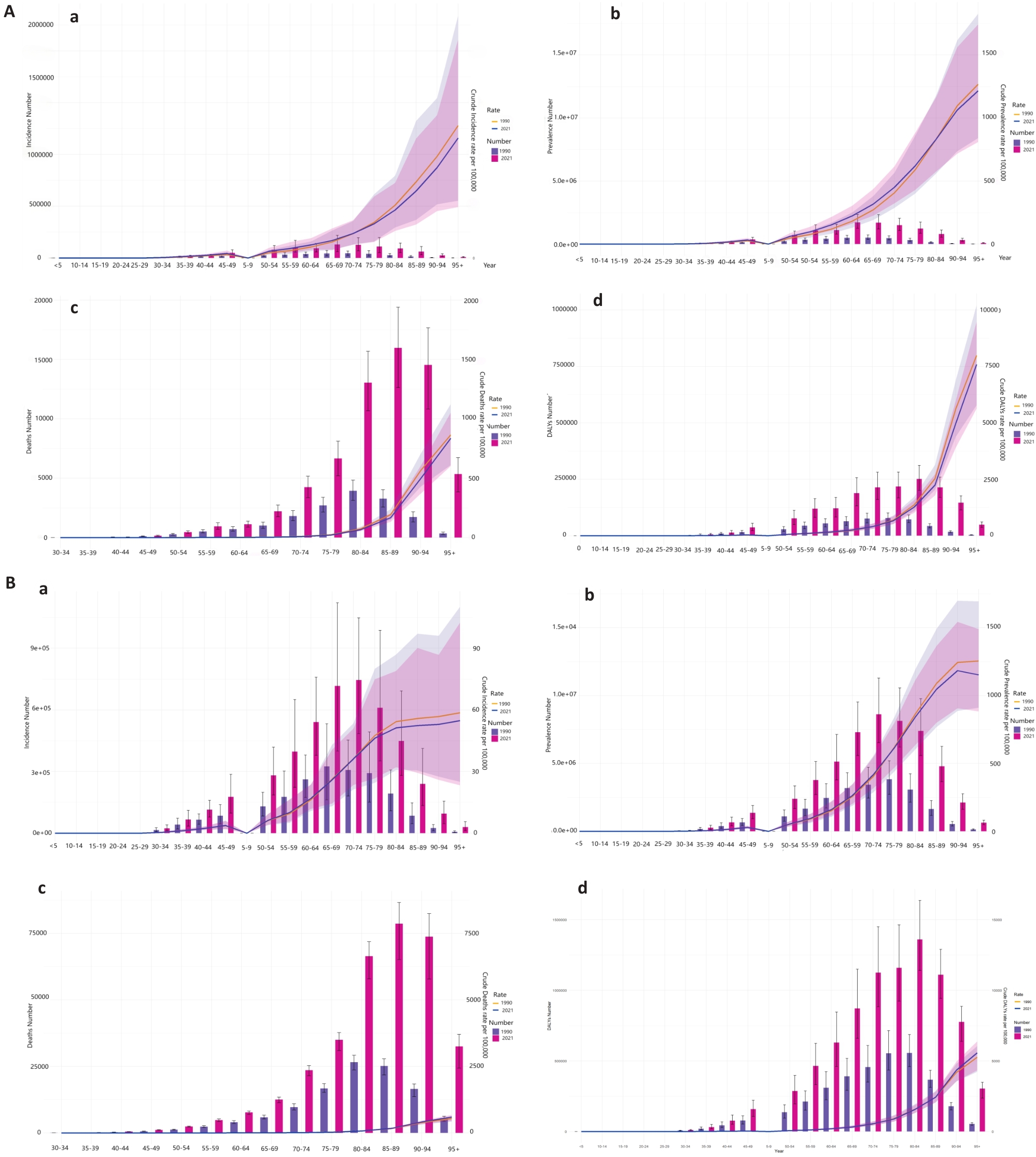
图3 1990年和2021年中国与全球按年龄组的发病率,患病率、死亡率和DALYs计数及其粗比率的比较
Fig.3 Comparative analyses of the incidence, prevalence, deaths, and DALYs counts, along with their crude rates, by age group in China and globally from 1990 and 2021. A: China. B: Global. (a) Incidence cases and CIR; (b) Prevalence cases and CMR; (c) Death cases and CMR; (d) DALYs counts and CDR. Bar charts represent counts; lines represent crude rates.

图4 1990年与2021中国和全球不同年龄组男女AF/AFL的发病率、患病率、死亡率和DALYs
Fig.4 Comparison of the incidence, prevalence, mortality, and DALYs of AF/AFL in males and females of different age groups in China and globally in 1990 and 2021. A: 1990 China. B: 2021 China. C: 1990 Global. D: 2021 Global. (a) Incidence; (b) Prevalence; (c) Deaths; (d) DALYs.
| Location | Year | High systolic blood pressure | Smoking | High alcohol | High BMI | High sodium diet | Low temperature |
|---|---|---|---|---|---|---|---|
| China | 1990 | 24.4% | 8.7% | 3.3% | 0.4% | 7.5% | 3.4% |
| 2021 | 29.8% | 6.9% | 3.7% | 4.5% | 6.6% | 3.4% | |
| Global | 1990 | 31.2% | 6.5% | 4.6% | 5.2% | 3.4% | 2.4% |
| 2021 | 30% | 4.7% | 4.3% | 8.7% | 3.4% | 2.7% |
表3 1990~2021年主要风险对年龄标准化AF/AFL死亡率百分比贡献
Tab.3 Percentage contributions of the major risk factors to age-standardized of AF/AFL
| Location | Year | High systolic blood pressure | Smoking | High alcohol | High BMI | High sodium diet | Low temperature |
|---|---|---|---|---|---|---|---|
| China | 1990 | 24.4% | 8.7% | 3.3% | 0.4% | 7.5% | 3.4% |
| 2021 | 29.8% | 6.9% | 3.7% | 4.5% | 6.6% | 3.4% | |
| Global | 1990 | 31.2% | 6.5% | 4.6% | 5.2% | 3.4% | 2.4% |
| 2021 | 30% | 4.7% | 4.3% | 8.7% | 3.4% | 2.7% |
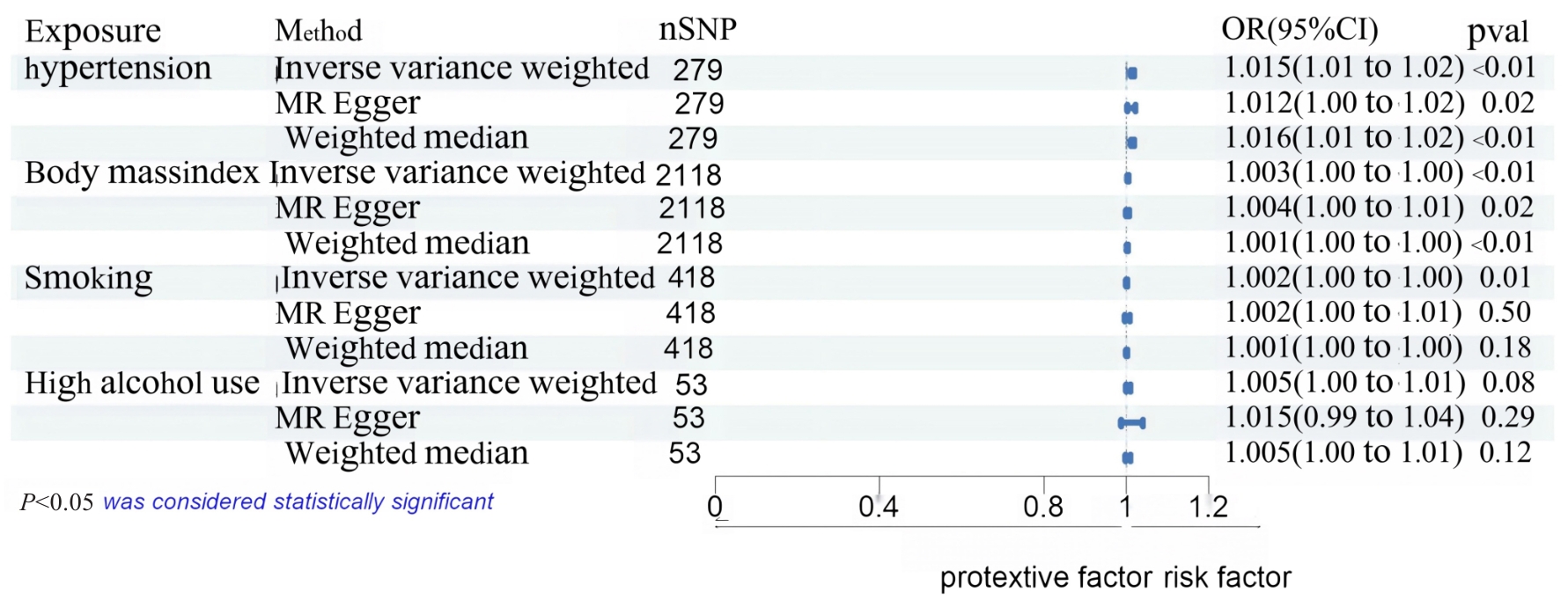
图5 危险因素与心房颤动/房扑发病危险性关系MR分析森林图
Fig.5 Forest plot of Mendelian randomization analysis for examining causal effects of the risk factors on AF/AFL incidence.
| [1] | Brundel BJJM, Ai X, Hills MT, et al. Atrial fibrillation[J]. Nat Rev Dis Primers, 2022, 8: 21. doi:10.1038/s41572-022-00347-9 |
| [2] | Reiffel JA. Atrial fibrillation: why are we hiding reality[J]?Circulation, 2024, 149(13): 979-80. doi:10.1161/circulationaha.123.067544 |
| [3] | Odutayo A, Wong CX, Hsiao AJ, et al. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: systematic review and meta-analysis[J]. BMJ, 2016, 354: i4482. doi:10.1136/bmj.i4482 |
| [4] | Writing Committee Members, Joglar JA, Chung MK, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines[J]. J Am Coll Cardiol, 2024, 83(1): 109-279. doi:10.1161/cir.0000000000001207 |
| [5] | Zimetbaum P. Atrial fibrillation[J]. Ann Intern Med, 2017, 166(5): ITC33-48. doi:10.7326/aitc201703070 |
| [6] | Heijman J, Linz D, Schotten U. Dynamics of atrial fibrillation mechanisms and comorbidities[J]. Annu Rev Physiol, 2021, 83: 83-106. doi:10.1146/annurev-physiol-031720-085307 |
| [7] | Antman EM, Leopold JA, Sauer WH, et al. Atrial fibrillation - what is it and how is it treated?[J]. N Engl J Med, 2022, 387(16): e38. doi:10.1056/nejmp2212939 |
| [8] | Elliott AD, Middeldorp ME, Van Gelder IC, et al. Author Correction: Epidemiology and modifiable risk factors for atrial fibrillation[J]. Nat Rev Cardiol, 2023, 20(6): 429. doi:10.1038/s41569-023-00834-w |
| [9] | Cheng SY, He JZ, Han YC, et al. Global burden of atrial fibrillation/atrial flutter and its attributable risk factors from 1990 to 2021[J]. Europace, 2024, 26(7): euae195. doi:10.1093/europace/euae195 |
| [10] | Dong XJ, Wang BB, Hou FF, et al. Global burden of atrial fibrillation/atrial flutter and its attributable risk factors from 1990 to 2019[J]. Europace, 2023,25(3):793-803. doi:10.1093/europace/euac237 |
| [11] | Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1204-22. |
| [12] | Foreman KJ, Lozano R, Lopez AD, et al. Modeling causes of death: an integrated approach using CODEm[J]. Popul Health Metr, 2012, 10: 1. doi:10.1186/1478-7954-10-1 |
| [13] | Stevens GA, Alkema L, Black RE, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement[J]. Lancet, 2016, 388(10062): e19-23. doi:10.1016/s0140-6736(16)30388-9 |
| [14] | Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomisation (STROBE-MR): explanation and elaboration[J]. BMJ, 2021, 375: n2233. doi:10.1136/bmj.n2233 |
| [15] | Sekula P, Fabiola Greco M, Pattaro C, et al. Mendelian randomization as an approach to assess causality using observational data[J]. J Am Soc Nephrol, 2016, 27(11): 3253-65. doi:10.1681/asn.2016010098 |
| [16] | Kim HJ, Fay MP, Feuer EJ, et al. Permutation tests for joinpoint regression with applications to cancer rates[J]. Stat Med, 2000, 19(3): 335-51. doi:10.1002/(sici)1097-0258(20000215)19:3<335::aid-sim336>3.3.co;2-q |
| [17] | Qiu HB, Cao SM, Xu RH. Cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with the United States and United Kingdom based on the global epidemiological data released in 2020[J]. Cancer Commun (Lond), 2021, 41(10): 1037-48. doi:10.1002/cac2.12197 |
| [18] | Lawlor DA, Harbord RM, Sterne JAC, et al. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology[J]. Stat Med, 2008, 27(8): 1133-63. doi:10.1002/sim.3034 |
| [19] | Barillas-Lara MI, Monahan K, Helm RH, et al. Sex-specific prevalence, incidence, and mortality associated with atrial fibrillation in heart failure[J]. JACC Clin Electrophysiol, 2021, 7(11): 1366-75. doi:10.1016/j.jacep.2021.02.021 |
| [20] | Benjamin EJ, Wolf PA, D'Agostino RB, et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study[J]. Circulation, 1998, 98(10): 946-52. doi:10.1161/01.cir.98.10.946 |
| [21] | Schnabel RB, Yin XY, Gona P, et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study[J]. Lancet, 2015, 386(9989): 154-62. doi:10.1016/s0140-6736(14)61774-8 |
| [22] | Tan SY, et al. Global, regional, and national burden of atrial fibrillation and atrial flutter from 1990 to 2021: sex differences and global burden projections to 2046: a systematic analysis of the Global Burden of Disease Study 2021[J]. Europace, 2025, 27(2): euaf027. doi:10.1093/europace/euaf027 |
| [23] | Buhari H, Fang JM, Han L, et al. Stroke risk in women with atrial fibrillation[J]. Eur Heart J, 2024, 45(2): 104-13. doi:10.1093/eurheartj/ehad508 |
| [24] | Gerdts E, Regitz-Zagrosek V. Sex differences in cardiometabolic disorders[J]. Nat Med, 2019, 25(11): 1657-66. doi:10.1038/s41591-019-0643-8 |
| [25] | Li X, Wu CQ, Lu JP, et al. Cardiovascular risk factors in China: a nationwide population-based cohort study[J]. Lancet Public Health, 2020, 5(12): e672-81. doi:10.1016/s2468-2667(20)30191-2 |
| [26] | Du X, Dong J, Ma C. Is atrial fibrillation a preventable disease?[J]. J Am Coll Cardiol, 2017, 69(15): 1968-82. doi:10.1016/j.jacc.2017.02.020 |
| [27] | O’Keefe EL, Sturgess JE, O’Keefe JH, et al. Prevention and treatment of atrial fibrillation via risk factor modification[J]. Am J Cardiol, 2021, 160: 46-52. doi:10.1016/j.amjcard.2021.08.042 |
| [28] | Oyama K, Raz I, Cahn A, et al. Obesity and effects of dapagliflozin on cardiovascular and renal outcomes in patients with type 2 diabetes mellitus in the DECLARE-TIMI 58 trial[J]. Eur Heart J, 2022, 43(31): 2958-67. doi:10.1093/eurheartj/ehab530 |
| [29] | Wilcox NS, Amit U, Reibel JB, et al. Cardiovascular disease and cancer: shared risk factors and mechanisms[J]. Nat Rev Cardiol, 2024, 21(9): 617-31. doi:10.1038/s41569-024-01017-x |
| [30] | Chung MK, Eckhardt LL, Chen LY, et al. Lifestyle and risk factor modification for reduction of atrial fibrillation: a scientific statement from the American heart association[J]. Circulation, 2020, 141(16): e750-72. doi:10.1161/cir.0000000000000748 |
| [31] | Lee KK, Doudesis D, Bing R, et al. Sex differences in oral anticoagulation therapy in patients hospitalized with atrial fibrillation: a nationwide cohort study[J]. J Am Heart Assoc, 2023, 12(5): e027211. doi:10.1161/jaha.122.027211 |
| [32] | Linde C, Bongiorni MG, Birgersdotter-Green U, et al. Sex differences in cardiac arrhythmia: a consensus document of the European heart rhythm association, endorsed by the heart rhythm society and Asia Pacific heart rhythm society[J]. Europace, 2018, 20(10): 1565-1565ao. doi:10.1093/europace/euy067 |
| [33] | Van Gelder IC, Rienstra M, Bunting KV, et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS)[J]. Eur Heart J, 2024, 45(36): 3314-414. |
| [34] | Parameswaran R, Al-Kaisey AM, Kalman JM. Catheter ablation for atrial fibrillation: current indications and evolving technologies[J]. Nat Rev Cardiol, 2021, 18(3): 210-25. doi:10.1038/s41569-020-00451-x |
| [35] | Ma CS, Wu SL, Liu SW, et al. Chinese guidelines for the diagnosis and management of atrial fibrillation[J]. J Geriatr Cardiol, 2024, 21(3): 251-314. doi:10.26599/1671-5411.2024.03.009 |
| [1] | 姜君, 封硕, 孙银贵, 安燕. 经尿道前列腺钬激光剜除术后低体温风险预测模型:基于逻辑回归、决策树和支持向量机[J]. 南方医科大学学报, 2025, 45(9): 2019-2025. |
| [2] | 刘倚彤, 赵克, 王晓东. 1990~2035年东亚地区唇与口腔癌的疾病负担分析及未来预测[J]. 南方医科大学学报, 2025, 45(7): 1554-1562. |
| [3] | 吕雪彩, 刘艳红, 韩诗怡, 张浩赟, 侯爱生, 周志康, 史立凯, 高洁, 曹江北, 张宏, 米卫东. 老年患者胃肠道手术后综合并发症的危险因素——一项多中心观察性研究[J]. 南方医科大学学报, 2025, 45(4): 736-743. |
| [4] | 李文婕, 洪耀南, 黄蕊, 李煜宸, 张莹, 张蕴, 吴迪炯. 自身免疫性疾病是再生障碍性贫血的危险因素:一项孟德尔随机化分析[J]. 南方医科大学学报, 2025, 45(4): 871-879. |
| [5] | 周莹, 张丹阳, 吴立凡, 王桂杉, 母杰丹, 崔成文, 石秀秀, 董继革, 王瑜, 许王莉, 李晓. 北京地区近10年骨质疏松症流行病学调查:一项单中心30 599例汉族人群双能X线吸收法骨密度检查结果分析[J]. 南方医科大学学报, 2025, 45(3): 443-452. |
| [6] | 高俊杰, 叶开, 吴竞. 槲皮素通过调控TP53基因抑制肾透明细胞癌的增殖和迁移[J]. 南方医科大学学报, 2025, 45(2): 313-321. |
| [7] | 邓颖, 张敏怡, 汪诗奥, 范顺昌, 陈佳琪, 冼举贤, 陈清. 1990~2021年全球5岁以下腹泻患儿的疾病负担分析及趋势预测[J]. 南方医科大学学报, 2025, 45(10): 2171-2181. |
| [8] | 姚辰, 李文佳, 庞瑞明, 周继红. 臀肌腱炎、原发性髋关节病可能导致髂胫束综合征—一项孟德尔随机化研究[J]. 南方医科大学学报, 2024, 44(9): 1821-1830. |
| [9] | 钟帷韬, 李伟松, 李泽霖, 王强, 张旺明. 睡眠性状与特发性正常压力脑积水的因果关联:一项两样本双向孟德尔随机化研究[J]. 南方医科大学学报, 2024, 44(8): 1612-1619. |
| [10] | 刘佳进, 缪长宏, 徐健康, 余伟杰, 陈继鑫, 唐好知, 刘爱峰. 肠道菌群与色素沉着绒毛结节性滑膜炎之间的因果关系:基于孟德尔随机化分析[J]. 南方医科大学学报, 2024, 44(7): 1397-1406. |
| [11] | 李和平, 李高桦, 张学华, 王亚楠. 直肠癌炎症蛋白因子的遗传驱动:孟德尔随机化方法在临床预后研究中的应用[J]. 南方医科大学学报, 2024, 44(7): 1361-1370. |
| [12] | 周勇, 吴媛, 曾汇文, 陈翠梅, 谢群, 贺莉萍. 艰难梭菌的感染特征及其危险因素:基于中南地区某市住院腹泻患者的标本[J]. 南方医科大学学报, 2024, 44(5): 998-1003. |
| [13] | 戈 悦, 李建伟, 梁宏开, 侯六生, 左六二, 陈 珍, 卢剑海, 赵 新, 梁静漪, 彭 岚, 包静娜, 段佳欣, 刘 俐, 毛可晴, 曾振华, 胡鸿彬, 陈仲清. VA-ECMO患者院内死亡风险预测模型的构建及验证:一项多中心、回顾性、病例对照研究[J]. 南方医科大学学报, 2024, 44(3): 491-498. |
| [14] | 胡嘉伟, 杜芳, 丁璐, 王路翔, 赵巍峰. 合并高血压病的乙型肝炎肝硬化患者发生肝细胞癌的风险评估:一项基于倾向性匹配评分的回顾性队列研究[J]. 南方医科大学学报, 2024, 44(11): 2243-2249. |
| [15] | 占雯婕, 赵 玲. 1型糖尿病可能增加甲状腺毒症的风险:基于两样本孟德尔随机化方法[J]. 南方医科大学学报, 2023, 43(8): 1396-1401. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||