Journal of Southern Medical University ›› 2025, Vol. 45 ›› Issue (2): 379-386.doi: 10.12122/j.issn.1673-4254.2025.02.19
Tianwei TANG1( ), Luan LI2, Yuanhan CHEN2, Li ZHANG2, Lixia XU2, Zhilian LI2, Zhonglin FENG2, Huilin ZHANG3, Ruifang HUA3, Zhiming YE2, Xinling LIANG2, Ruizhao LI1()
), Luan LI2, Yuanhan CHEN2, Li ZHANG2, Lixia XU2, Zhilian LI2, Zhonglin FENG2, Huilin ZHANG3, Ruifang HUA3, Zhiming YE2, Xinling LIANG2, Ruizhao LI1()
Received:2024-08-17
Online:2025-02-20
Published:2025-03-03
Contact:
Ruizhao LI
E-mail:tw122666@163.com;liruizhao1979@126.com
Tianwei TANG, Luan LI, Yuanhan CHEN, Li ZHANG, Lixia XU, Zhilian LI, Zhonglin FENG, Huilin ZHANG, Ruifang HUA, Zhiming YE, Xinling LIANG, Ruizhao LI. High serum cystatin C is an independent risk factor for poor renal prognosis in IgA nephropathy[J]. Journal of Southern Medical University, 2025, 45(2): 379-386.
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.j-smu.com/EN/10.12122/j.issn.1673-4254.2025.02.19
| Pathological parameters and score | Content |
|---|---|
| Mesangial hypercellularity (M) | |
| M0 | Mesangial score ≤0.5 |
| M1 | Mesangial score >0.5 |
| Endocapillary hypercellularity (E) | |
| E0 | Absent |
| E1 | Present |
| Segmental glomerulosclerosis (S) | |
| S0 | Absent |
| S1 | Present |
| Tubular atrophy/interstitial fibrosis (T) | |
| T0 | 0-25% |
| T1 | 26%-50% |
| T2 | >50% |
| Cellular/fibrocellular crescents (C) | |
| C0 | Absent |
| C1 | Crescents in a least 1 glomerulus and <25% of glomeruli |
| C2 | Crescents in ≥25% of glomeruli |
Tab.1 Oxford Classification of IgA nephropathy (MEST-C score)
| Pathological parameters and score | Content |
|---|---|
| Mesangial hypercellularity (M) | |
| M0 | Mesangial score ≤0.5 |
| M1 | Mesangial score >0.5 |
| Endocapillary hypercellularity (E) | |
| E0 | Absent |
| E1 | Present |
| Segmental glomerulosclerosis (S) | |
| S0 | Absent |
| S1 | Present |
| Tubular atrophy/interstitial fibrosis (T) | |
| T0 | 0-25% |
| T1 | 26%-50% |
| T2 | >50% |
| Cellular/fibrocellular crescents (C) | |
| C0 | Absent |
| C1 | Crescents in a least 1 glomerulus and <25% of glomeruli |
| C2 | Crescents in ≥25% of glomeruli |
| Variables | Overall (n=356) | Normal serum CysC group (n=130) | High serum CysC group (n=226) | t/Z/χ2 | P |
|---|---|---|---|---|---|
| Age (year) | 36 (29, 45) | 32 (26, 39) | 39 (32, 47) | -5.245 | <0.001 |
| Male [n (%)] | 149 (41.9) | 33(25.4) | 116 (51.3) | 21.770 | <0.001 |
| Hypertension [n (%)] | 139 (39.0) | 28 (21.5) | 111 (49.1) | 25.224 | <0.001 |
| Hyperuricaemia [n (%)] | 31 ( 8.7) | 5 (3.8) | 26 (11.5) | 5.163 | 0.023 |
| Mean arterial pressure (mmHg) | 100.34 (91, 112.34) | 94.67 (87.33, 104.33) | 105 (94.67, 115.25) | -5.989 | <0.001 |
| Weight (kg) | 59.8 (52.39, 68) | 58 (51, 65.81) | 61.48 (53.78, 69.48) | -2.766 | 0.006 |
| Serum uric acid (μmol/L) | 423.5 (342, 517.5) | 345 (293, 409) | 470.1 (392.25, 565) | -9.559 | <0.001 |
| Serum sodium (mmol/L) | 139 (137.7, 140.5) | 138.9 (137.7, 140.2) | 139.1 (137.8, 140.7) | -0.794 | 0.427 |
| Serum potassium (mmol/L) | 3.72 (3.49, 3.95) | 3.58 (3.4, 3.77) | 3.84 (3.58, 4.07) | -6.489 | <0.001 |
| Serum albumin (g/L) | 36.7 (33.78, 39.8) | 37.35 (34.53, 40.78) | 36.3 (32.4, 39.1) | 3.049 | 0.002 |
| Triglyceride (mmol/L) | 1.59 (1.11, 2.49) | 1.38 (0.98, 2.02) | 1.78 (1.25, 2.57) | -3.577 | <0.001 |
| Cholesterol (mmol/L) | 5.3 (4.4, 6.04) | 5.15 (4.25, 5.68) | 5.36 (4.56, 6.29) | -2.544 | 0.011 |
| Low density lipoprotein cholesterol (mmol/L) | 3.19 (2.62, 3.89) | 3.1 (2.49, 3.53) | 3.27 (2.65, 4.04) | -2.777 | 0.005 |
| High density lipoprotein cholesterol (mmol/L) | 1.15 (0.96, 1.41) | 1.23 (1.01, 1.48) | 1.13 (0.93, 1.38) | 2.306 | 0.021 |
| Transferrin (g/L) | 1.96 (1.76, 2.25) | 2.11 (1.85, 2.36) | 1.91 (1.73, 2.17) | 4.300 | <0.001 |
| Serum IgA (g/L) | 3.4 (2.5, 4.09) | 3.23 (2.49, 3.79) | 3.47 (2.55, 4.45) | -1.908 | 0.056 |
| Serum IgM (g/L) | 1.16 (0.83, 1.68) | 1.21 (0.88, 1.67) | 1.14 (0.8, 1.68) | 1.154 | 0.249 |
| Serum IgG (g/L) | 11.5 (9.74, 13.1) | 11.4 (10.1, 12.6) | 11.55 (9.6, 13.5) | -0.551 | 0.582 |
| Complement C3 (mg/L) | 878 (773.75, 1010) | 889 (769.25, 1010) | 868 (776.5, 1000) | 0.592 | 0.555 |
| Complement C4 (mg/L) | 226 (178, 275) | 215.5 (166.25, 250.5) | 233 (184.5, 284) | -2.971 | 0.003 |
| Hemoglobin (g/L) | 124.56±18.02 | 126.68±16.16 | 123.34±18.92 | 1.765 | 0.079 |
| White blood cell (×109/L) | 7.48 (6.41, 8.69) | 7.37 (6.31, 8.59) | 7.59 (6.51, 8.75) | -1.049 | 0.295 |
| Platelet (×109/L) | 251 (209, 289.25) | 256.5 (218, 296) | 249 (204, 285.75) | 1.685 | 0.092 |
| Fibrinogen (g/L) | 3.56 (3.08, 4.31) | 3.31 (2.91, 3.85) | 3.73 (3.16, 4.54) | -4.052 | <0.001 |
| D-Dimer(ng/mL) | 330 (270, 472.5) | 290 (270, 390) | 350 (270, 520) | -3.168 | 0.001 |
| Hematuria [n (%)] | 151 (42.4) | 78 (60.0) | 73 (32.3) | 24.802 | <0.001 |
| 24 h urine protein (g) | 1.14 (0.51, 2.16) | 0.70 (0.33, 1.40) | 1.38 (0.69, 2.67) | -5.977 | <0.001 |
| eGFR[mL·min-1·(1.73 m2)-1] | 65.62 (39.43, 100.51) | 106.39 (88.53, 119.9) | 44.84 (31.57, 64.36) | 13.664 | <0.001 |
| Serum IgA/Complement C3 | 3.68 (2.83, 4.76) | 3.61 (2.75, 4.34) | 3.8 (2.86, 5.09) | -1.785 | 0.074 |
| RAAS-inhibitor [n (%)] | 294 (82.6) | 125 (96.2) | 169 (74.8) | 24.752 | <0.001 |
| Immunosuppressive agents [n (%)] | 217 (61.0) | 64 (49.2) | 153 (67.7) | 11.064 | 0.001 |
| Percentage of global glomerulosclerosis | 0.23 (0.09, 0.46) | 0.1 (0.03, 0.18) | 0.36 (0.17, 0.55) | -9.405 | <0.001 |
| M1 [n (%)] | 291 (81.7) | 110 (84.6) | 181 (80.1) | 0.850 | 0.357 |
| E1 [n (%)] | 54 (15.2) | 22 (16.9) | 32 (14.2) | 0.299 | 0.585 |
| S1 [n (%)] | 167 (46.9) | 49 (37.7) | 118 (52.2) | 6.416 | 0.011 |
| T [n (%)] | 92.316 | <0.001 | |||
| 0 | 209 (58.7) | 119 (91.5) | 90 (39.8) | ||
| 1 | 91 (25.6) | 10 (7.7) | 81 (35.8) | ||
| 2 | 56 (15.7) | 1 (0.8) | 55 (24.3) | ||
| C [n (%)] | 7.860 | 0.020 | |||
| 0 | 152 (42.7) | 49 (37.7) | 103 (45.6) | ||
| 1 | 168 (47.2) | 73 (56.2) | 95 (42.0) | ||
| 2 | 36 (10.1) | 8 (6.2) | 28 (12.4) |
Tab.2 Baseline data of the patients with normal and high serum CysC levels
| Variables | Overall (n=356) | Normal serum CysC group (n=130) | High serum CysC group (n=226) | t/Z/χ2 | P |
|---|---|---|---|---|---|
| Age (year) | 36 (29, 45) | 32 (26, 39) | 39 (32, 47) | -5.245 | <0.001 |
| Male [n (%)] | 149 (41.9) | 33(25.4) | 116 (51.3) | 21.770 | <0.001 |
| Hypertension [n (%)] | 139 (39.0) | 28 (21.5) | 111 (49.1) | 25.224 | <0.001 |
| Hyperuricaemia [n (%)] | 31 ( 8.7) | 5 (3.8) | 26 (11.5) | 5.163 | 0.023 |
| Mean arterial pressure (mmHg) | 100.34 (91, 112.34) | 94.67 (87.33, 104.33) | 105 (94.67, 115.25) | -5.989 | <0.001 |
| Weight (kg) | 59.8 (52.39, 68) | 58 (51, 65.81) | 61.48 (53.78, 69.48) | -2.766 | 0.006 |
| Serum uric acid (μmol/L) | 423.5 (342, 517.5) | 345 (293, 409) | 470.1 (392.25, 565) | -9.559 | <0.001 |
| Serum sodium (mmol/L) | 139 (137.7, 140.5) | 138.9 (137.7, 140.2) | 139.1 (137.8, 140.7) | -0.794 | 0.427 |
| Serum potassium (mmol/L) | 3.72 (3.49, 3.95) | 3.58 (3.4, 3.77) | 3.84 (3.58, 4.07) | -6.489 | <0.001 |
| Serum albumin (g/L) | 36.7 (33.78, 39.8) | 37.35 (34.53, 40.78) | 36.3 (32.4, 39.1) | 3.049 | 0.002 |
| Triglyceride (mmol/L) | 1.59 (1.11, 2.49) | 1.38 (0.98, 2.02) | 1.78 (1.25, 2.57) | -3.577 | <0.001 |
| Cholesterol (mmol/L) | 5.3 (4.4, 6.04) | 5.15 (4.25, 5.68) | 5.36 (4.56, 6.29) | -2.544 | 0.011 |
| Low density lipoprotein cholesterol (mmol/L) | 3.19 (2.62, 3.89) | 3.1 (2.49, 3.53) | 3.27 (2.65, 4.04) | -2.777 | 0.005 |
| High density lipoprotein cholesterol (mmol/L) | 1.15 (0.96, 1.41) | 1.23 (1.01, 1.48) | 1.13 (0.93, 1.38) | 2.306 | 0.021 |
| Transferrin (g/L) | 1.96 (1.76, 2.25) | 2.11 (1.85, 2.36) | 1.91 (1.73, 2.17) | 4.300 | <0.001 |
| Serum IgA (g/L) | 3.4 (2.5, 4.09) | 3.23 (2.49, 3.79) | 3.47 (2.55, 4.45) | -1.908 | 0.056 |
| Serum IgM (g/L) | 1.16 (0.83, 1.68) | 1.21 (0.88, 1.67) | 1.14 (0.8, 1.68) | 1.154 | 0.249 |
| Serum IgG (g/L) | 11.5 (9.74, 13.1) | 11.4 (10.1, 12.6) | 11.55 (9.6, 13.5) | -0.551 | 0.582 |
| Complement C3 (mg/L) | 878 (773.75, 1010) | 889 (769.25, 1010) | 868 (776.5, 1000) | 0.592 | 0.555 |
| Complement C4 (mg/L) | 226 (178, 275) | 215.5 (166.25, 250.5) | 233 (184.5, 284) | -2.971 | 0.003 |
| Hemoglobin (g/L) | 124.56±18.02 | 126.68±16.16 | 123.34±18.92 | 1.765 | 0.079 |
| White blood cell (×109/L) | 7.48 (6.41, 8.69) | 7.37 (6.31, 8.59) | 7.59 (6.51, 8.75) | -1.049 | 0.295 |
| Platelet (×109/L) | 251 (209, 289.25) | 256.5 (218, 296) | 249 (204, 285.75) | 1.685 | 0.092 |
| Fibrinogen (g/L) | 3.56 (3.08, 4.31) | 3.31 (2.91, 3.85) | 3.73 (3.16, 4.54) | -4.052 | <0.001 |
| D-Dimer(ng/mL) | 330 (270, 472.5) | 290 (270, 390) | 350 (270, 520) | -3.168 | 0.001 |
| Hematuria [n (%)] | 151 (42.4) | 78 (60.0) | 73 (32.3) | 24.802 | <0.001 |
| 24 h urine protein (g) | 1.14 (0.51, 2.16) | 0.70 (0.33, 1.40) | 1.38 (0.69, 2.67) | -5.977 | <0.001 |
| eGFR[mL·min-1·(1.73 m2)-1] | 65.62 (39.43, 100.51) | 106.39 (88.53, 119.9) | 44.84 (31.57, 64.36) | 13.664 | <0.001 |
| Serum IgA/Complement C3 | 3.68 (2.83, 4.76) | 3.61 (2.75, 4.34) | 3.8 (2.86, 5.09) | -1.785 | 0.074 |
| RAAS-inhibitor [n (%)] | 294 (82.6) | 125 (96.2) | 169 (74.8) | 24.752 | <0.001 |
| Immunosuppressive agents [n (%)] | 217 (61.0) | 64 (49.2) | 153 (67.7) | 11.064 | 0.001 |
| Percentage of global glomerulosclerosis | 0.23 (0.09, 0.46) | 0.1 (0.03, 0.18) | 0.36 (0.17, 0.55) | -9.405 | <0.001 |
| M1 [n (%)] | 291 (81.7) | 110 (84.6) | 181 (80.1) | 0.850 | 0.357 |
| E1 [n (%)] | 54 (15.2) | 22 (16.9) | 32 (14.2) | 0.299 | 0.585 |
| S1 [n (%)] | 167 (46.9) | 49 (37.7) | 118 (52.2) | 6.416 | 0.011 |
| T [n (%)] | 92.316 | <0.001 | |||
| 0 | 209 (58.7) | 119 (91.5) | 90 (39.8) | ||
| 1 | 91 (25.6) | 10 (7.7) | 81 (35.8) | ||
| 2 | 56 (15.7) | 1 (0.8) | 55 (24.3) | ||
| C [n (%)] | 7.860 | 0.020 | |||
| 0 | 152 (42.7) | 49 (37.7) | 103 (45.6) | ||
| 1 | 168 (47.2) | 73 (56.2) | 95 (42.0) | ||
| 2 | 36 (10.1) | 8 (6.2) | 28 (12.4) |
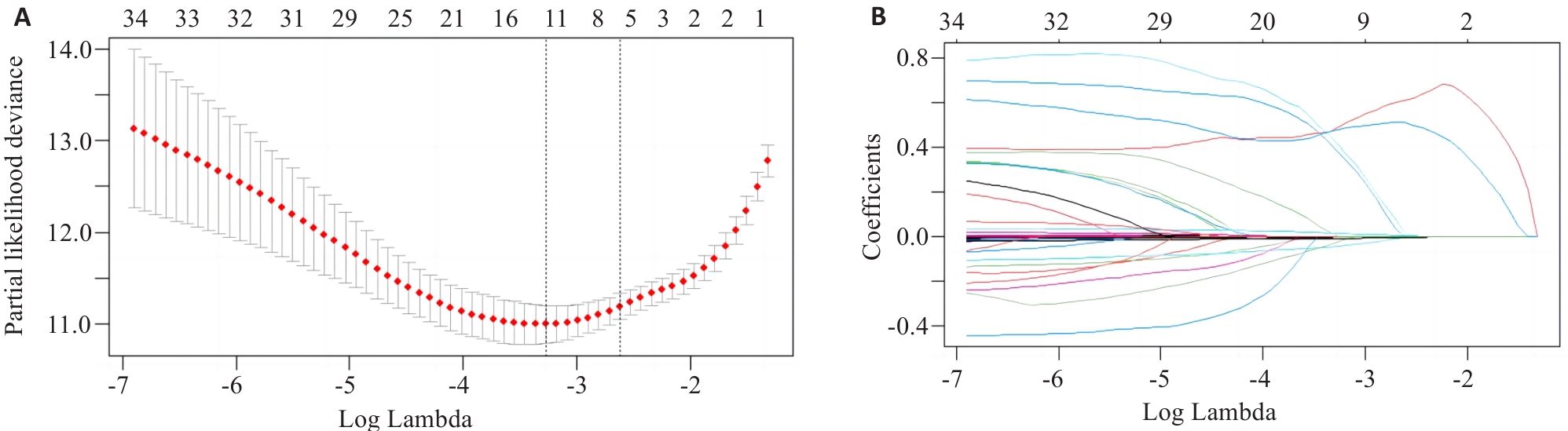
Fig.1 Variable selection by Lasso regression model. A: Log Lambda versus partial likelihood deviance. B: Log Lambda versus coefficients.
| Variables | Lasso regression coefficients | Multivariate Cox regression | |
|---|---|---|---|
| HR (95% CI) | P | ||
| Mean arterial pressure (mmHg) | 4.23×10-3 | 1.015 (1.000-1.031) | 0.048 |
| Serum CysC (mg/L) | 6.10×10-1 | 2.142 (1.222-3.755) | 0.008 |
| Serum albumin (g/L) | -4.57×10-3 | 0.934 (0.892-0.977) | 0.003 |
| 24-hour urine protein (g) | 2.88×10-5 | 1.000 (0.999-1.000) | 0.638 |
| eGFR[mL·min-1·(1.73 m2)-1] | -5.43×10-3 | 0.984 (0.965-1.003) | 0.107 |
| Percentage of global glomerulosclerosis | 1.81×10-2 | 2.077 (0.518-8.327) | 0.302 |
| T [n (%)] | 5.10×10-1 | 1.000 (Ref) | |
| T1 | 3.416 (1.424-8.192) | 0.006 | |
| T2 | 3.408 (1.144-10.150) | 0.028 | |
Tab.3 Lasso regression and multivariate Cox regression analysis of the risk factors for poor renal prognosis in IgAN
| Variables | Lasso regression coefficients | Multivariate Cox regression | |
|---|---|---|---|
| HR (95% CI) | P | ||
| Mean arterial pressure (mmHg) | 4.23×10-3 | 1.015 (1.000-1.031) | 0.048 |
| Serum CysC (mg/L) | 6.10×10-1 | 2.142 (1.222-3.755) | 0.008 |
| Serum albumin (g/L) | -4.57×10-3 | 0.934 (0.892-0.977) | 0.003 |
| 24-hour urine protein (g) | 2.88×10-5 | 1.000 (0.999-1.000) | 0.638 |
| eGFR[mL·min-1·(1.73 m2)-1] | -5.43×10-3 | 0.984 (0.965-1.003) | 0.107 |
| Percentage of global glomerulosclerosis | 1.81×10-2 | 2.077 (0.518-8.327) | 0.302 |
| T [n (%)] | 5.10×10-1 | 1.000 (Ref) | |
| T1 | 3.416 (1.424-8.192) | 0.006 | |
| T2 | 3.408 (1.144-10.150) | 0.028 | |
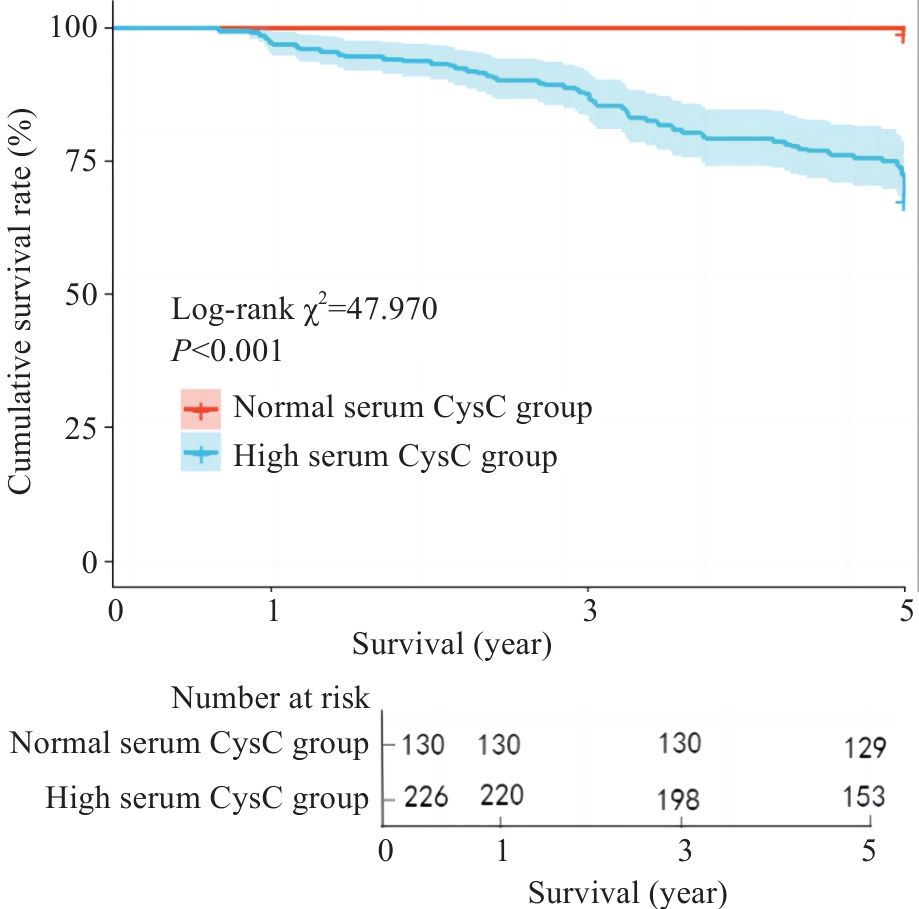
Fig.2 Kaplan-Meier survival curves for analyzing the effect of serum CysC on 5-year renal survival rate of IgAN patients.
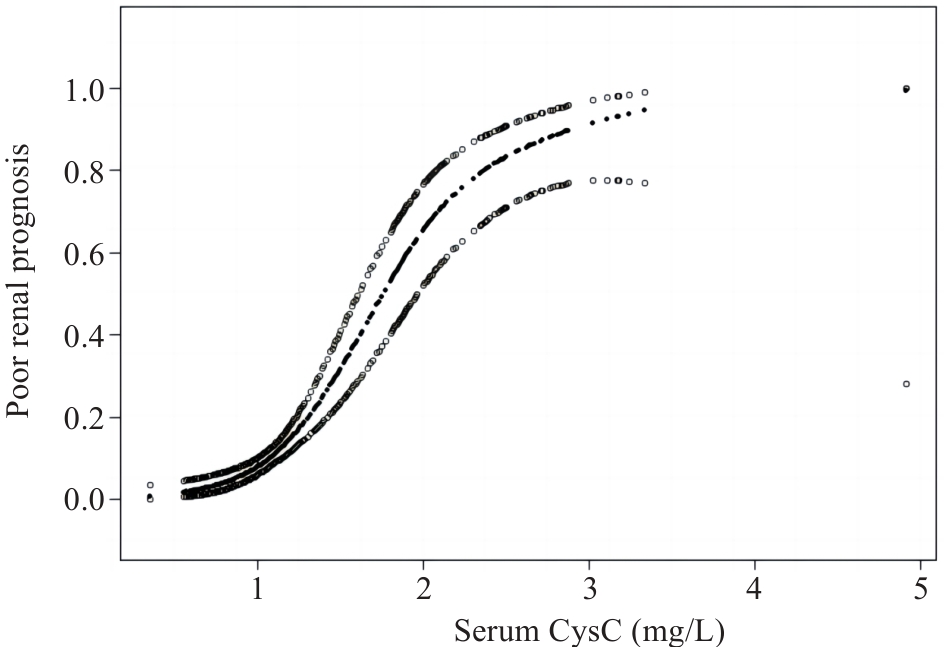
Fig.3 Generalized additive models demonstrate the relationship between serum CysC level and poor renal prognosis of IgAN.
| Threshold effect | β (95% CI) | P |
|---|---|---|
| Fitting by GAMs | ||
| Serum CysC | 2.637 (2.034, 3.240) | <0.001 |
| Fitting by two-piecewise GAMs | ||
| Inflection point | 2.12 | |
| Serum CysC≤2.12 | 3.487 (2.561, 4.413) | <0.001 |
| Serum CysC>2.12 | 0.676 (-0.642, 1.995) | 0.315 |
| Log likelihood ratio | 0.008 |
Tab.4 Threshold effect analysis of serum CysC level and poor renal prognosis of IgAN
| Threshold effect | β (95% CI) | P |
|---|---|---|
| Fitting by GAMs | ||
| Serum CysC | 2.637 (2.034, 3.240) | <0.001 |
| Fitting by two-piecewise GAMs | ||
| Inflection point | 2.12 | |
| Serum CysC≤2.12 | 3.487 (2.561, 4.413) | <0.001 |
| Serum CysC>2.12 | 0.676 (-0.642, 1.995) | 0.315 |
| Log likelihood ratio | 0.008 |
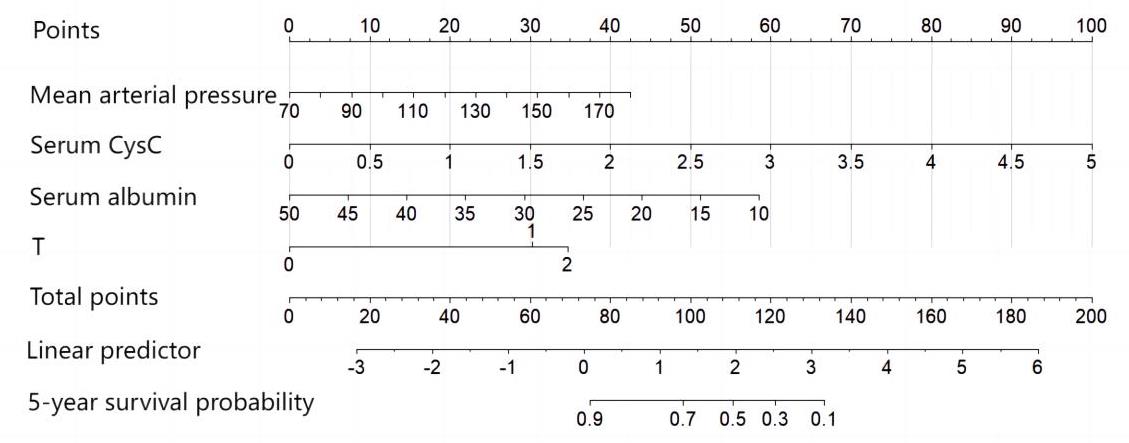
Fig.4 Nomogram prediction model of the prognosis of IgAN patients.
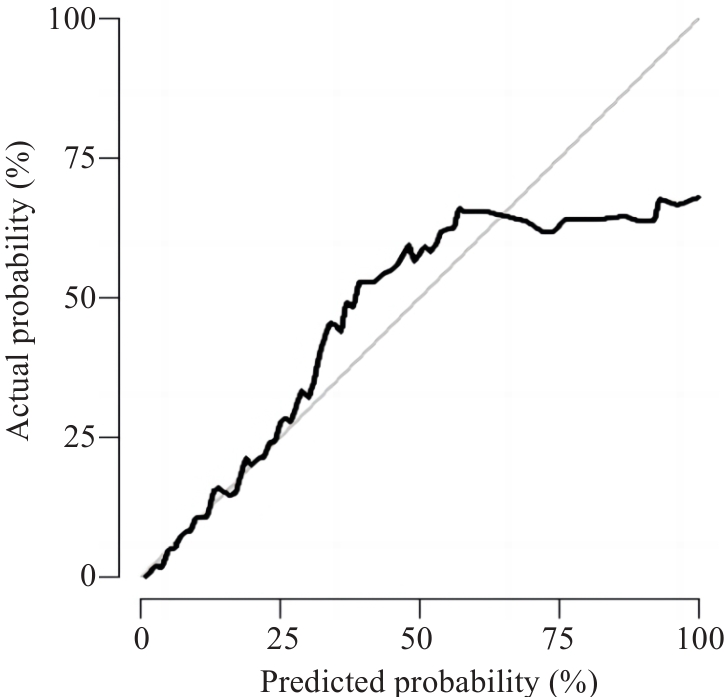
Fig.5 Calibration curve of nomogram prediction model.
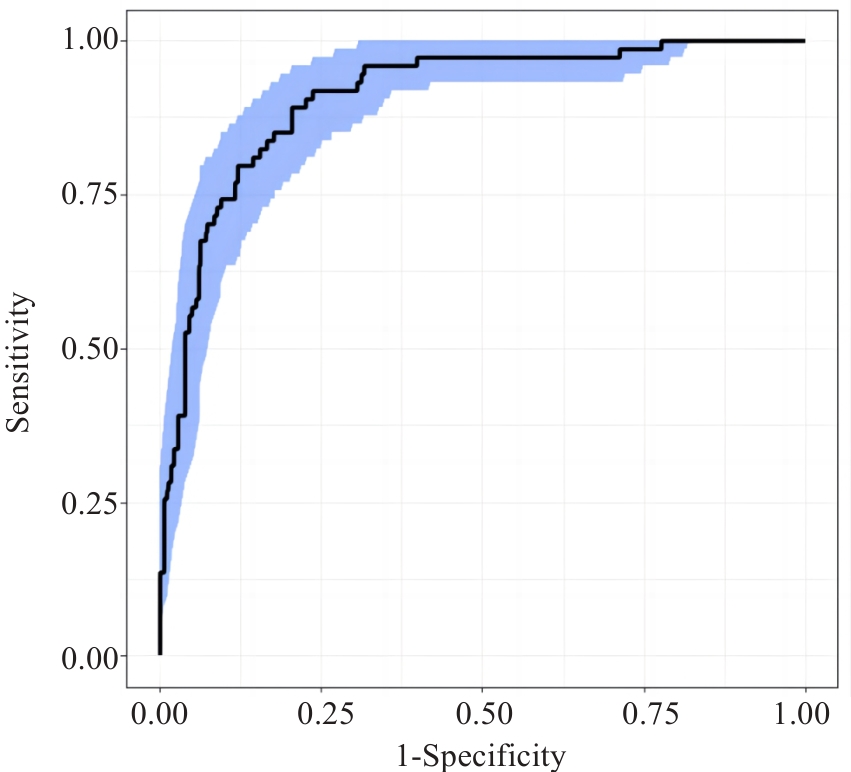
Fig.6 ROC curve of nomogram prediction model.
| 1 | Lai KN, Tang SC, Schena FP, et al. IgA nephropathy[J]. Nat Rev Dis Primers, 2016, 2: 16001. |
| 2 | DiseaseKidney: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 clinical practice guideline for the management of glomerular diseases[J]. Kidney Int, 2021, 100(4s): S1-276. |
| 3 | Spencer S, Desborough R, Bhandari S. Should cystatin C eGFR become routine clinical practice[J]. Biomolecules, 2023, 13(7): 1075. |
| 4 | Feng BY, Lu Y, Ye L, et al. Mendelian randomization study supports the causal association between serum cystatin C and risk of diabetic nephropathy[J]. Front Endocrinol, 2022, 13: 1043174. |
| 5 | Chen SH, Tang YZ, Zhou XY. Cystatin C for predicting all-cause mortality and rehospitalization in patients with heart failure: a meta-analysis[J]. Biosci Rep, 2019, 39(2): BSR20181761. |
| 6 | Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race[J]. N Engl J Med, 2021, 385(19): 1737-49. |
| 7 | Trimarchi H, Barratt J, Cattran DC, et al. Oxford classification of IgA nephropathy 2016: an update from the IgA nephropathy classification working group[J]. Kidney Int, 2017, 91(5): 1014-21. |
| 8 | Dejenie TA, Abebe EC, Mengstie MA, et al. Dyslipidemia and serum cystatin C levels as biomarker of diabetic nephropathy in patients with type 2 diabetes mellitus[J]. Front Endocrinol, 2023, 14: 1124367. |
| 9 | Séronie-Vivien S, Delanaye P, Piéroni L, et al. Cystatin C: current position and future prospects[J]. Clin Chem Lab Med, 2008, 46(12): 1664-86. |
| 10 | Zou LX, Sun L, Nicholas SB, et al. Comparison of bias and accuracy using cystatin C and creatinine in CKD-EPI equations for GFR estimation[J]. Eur J Intern Med, 2020, 80: 29-34. |
| 11 | Liao XL, Zhu Y, Xue C. Diagnostic value of serum cystatin C for diabetic nephropathy: a meta-analysis[J]. BMC Endocr Disord, 2022, 22(1): 149. |
| 12 | 曾思权. 血清胱抑素C测定在原发性高血压早期肾损伤中的诊断价值[J]. 中国医学工程, 2016, 24(9): 40-2. |
| 13 | 蔡 萍. CysC水平变化在早期诊断急性肾损伤中的价值[J]. 四川医学, 2016, 37(4): 438-40. |
| 14 | Wali U, Hussain MM, Wali N, et al. Comparison of serum levels of Cystatin-C and traditional renal biomarkers for the early detection of pre-hypertensive nephropathy[J]. J Pak Med Assoc, 2019, 69(3): 313-9. |
| 15 | 蔡小凡, 符欣漪, 蔡秀峰, 等. 血清胱抑素C水平与IgA肾病临床及病理特征的相关性[J]. 中华检验医学杂志, 2022, 45(9): 957-62. |
| 16 | 陆 放, 张承宁, 段俗言, 等. 血清胱抑素C水平评估2型糖尿病患者肾病预后的价值[J]. 中华检验医学杂志, 2023, 46(4): 375-84. |
| 17 | Chen TY, Li X, Li YX, et al. Prediction and risk stratification of kidney outcomes in IgA nephropathy[J]. Am J Kidney Dis, 2019, 74(3): 300-9. |
| 18 | Xie JY, Lv JC, Wang WM, et al. Kidney failure risk prediction equations in IgA nephropathy: a multicenter risk assessment study in Chinese patients[J]. Am J Kidney Dis, 2018, 72(3): 371-80. |
| 19 | Zi MT, Xu YK. Involvement of cystatin C in immunity and apoptosis[J]. Immunol Lett, 2018, 196: 80-90. |
| 20 | Xu YK, Ding Y, Li XC, et al. Cystatin C is a disease-associated protein subject to multiple regulation[J]. Immunol Cell Biol, 2015, 93(5): 442-51. |
| 21 | 郭唯一, 安秀平, 孙丽君, 等. 伴肾小动脉硬化病变的IgA肾病的临床病理特点及预后[J]. 中华肾脏病杂志, 2023, 39(3): 209-14. |
| 22 | Sugiura N, Moriyama T, Miyabe Y, et al. Severity of arterial and/or arteriolar sclerosis in IgA nephropathy and the effects of renin-angiotensin system inhibitors on its prognosis[J]. J Pathol Clin Res, 2021, 7(6): 616-23. |
| 23 | Peng W, Tang Y, Tan L, et al. Crescents and global glomerulosclerosis in Chinese IgA nephropathy patients: a five-year follow-up[J]. Kidney Blood Press Res, 2019, 44(1): 103-12. |
| 24 | Lee K, Shin J, Park J, et al. First-year GFR slope and long-term renal outcome in IgA nephropathy[J]. Eur J Clin Invest, 2018, 48(6): e12936. |
| 25 | Le WB, Liang SS, Hu YL, et al. Long-term renal survival and related risk factors in patients with IgA nephropathy: results from a cohort of 1155 cases in a Chinese adult population[J]. Nephrol Dial Transplant, 2012, 27(4): 1479-85. |
| 26 | Bartosik LP, Lajoie G, Sugar L, et al. Predicting progression in IgA nephropathy[J]. Am J Kidney Dis, 2001, 38(4): 728-35. |
| 27 | 袁燕红, 王 琴, 张敏芳, 等. 血清白蛋白对IgA肾病患者肾脏预后的预测价值[J]. 中华肾脏病杂志, 2015, 31(2): 102-8. |
| 28 | 卢清梅, 潘 玲, 莫曼秋, 等. 同型半胱氨酸预测IgA肾病患者肾脏预后不良的价值[J]. 中华肾脏病杂志, 2022, 38(8): 718-21. |
| 29 | 唐天威, 叶智明, 李锐钊. IgA肾病预后的影响因素及相关评估模型的研究进展[J]. 中华肾脏病杂志, 2024, 40(6): 499-505. |
| 30 | Xie JY, Kiryluk K, Wang WM, et al. Predicting progression of IgA nephropathy: new clinical progression risk score[J]. PLoS One, 2012, 7(6): e38904. |
| 31 | Zhu XJ, Li HQ, Liu YX, et al. Tubular atrophy/interstitial fibrosis scores of Oxford classification combinded with proteinuria level at biopsy provides earlier risk prediction in lgA nephropathy[J]. Sci Rep, 2017, 7(1): 1100. |
| 32 | Coppo R, Troyanov S, Bellur S, et al. Validation of the Oxford classification of IgA nephropathy in cohorts with different presentations and treatments[J]. Kidney Int, 2014, 86(4): 828-36. |
| [1] | Xue SONG, Yue CHEN, Min ZHANG, Nuo ZHANG, Lugen ZUO, Jing LI, Zhijun GENG, Xiaofeng ZHANG, Yueyue WANG, Lian WANG, Jianguo HU. GPSM2 is highly expressed in gastric cancer to affect patient prognosis by promoting tumor cell proliferation [J]. Journal of Southern Medical University, 2025, 45(2): 229-238. |
| [2] | Xiaorui CHEN, Qingzheng WEI, Zongliang ZHANG, Jiangshui YUAN, Weiqing SONG. Overexpression of CHMP2B suppresses proliferation of renal clear cell carcinoma cells [J]. Journal of Southern Medical University, 2025, 45(1): 126-136. |
| [3] | Yaobin WANG, Liuyan CHEN, Yiling LUO, Jiqing SHEN, Sufang ZHOU. Predictive value of NUF2 for prognosis and immunotherapy responses in pan-cancer [J]. Journal of Southern Medical University, 2025, 45(1): 137-149. |
| [4] | Chao ZHOU, Jingjing ZHANG, Qiao TANG, Shuangnan FU, Ning ZHANG, Zhaoyun HE, Jin ZHANG, Tianyi ZHANG, Pengcheng LIU, Man GONG. Value of serum tryptophan in stratified management of 90-day mortality risk in patients with hepatitis B virus-related acute-on-chronic liver failure: a multicenter retrospective study [J]. Journal of Southern Medical University, 2025, 45(1): 59-64. |
| [5] | Xiaohua CHEN, Hui LU, Ziliang WANG, Lian WANG, Yongsheng XIA, Zhijun GENG, Xiaofeng ZHANG, Xue SONG, Yueyue WANG, Jing LI, Jianguo HU, Lugen ZUO. Role of Abelson interactor 2 in progression and prognosis of gastric cancer and its regulatory mechanisms [J]. Journal of Southern Medical University, 2024, 44(9): 1653-1661. |
| [6] | Mengnan YE, Hongmei WU, Yan MEI, Qingling ZHANG. High expression of CREM is associated with poor prognosis in gastric cancer patients [J]. Journal of Southern Medical University, 2024, 44(9): 1776-1782. |
| [7] | Kai JI, Guanyu YU, Leqi ZHOU, Tianshuai ZHANG, Qianlong LING, Wenjiang MAN, Bing ZHU, Wei ZHANG. HNRNPA1 gene is highly expressed in colorectal cancer: its prognostic implications and potential as a therapeutic target [J]. Journal of Southern Medical University, 2024, 44(9): 1685-1695. |
| [8] | Jingjing YANG, Lixia YIN, Ting DUAN, Minzhu NIU, Zhendong HE, Xinrui CHEN, Xiaofeng ZHANG, Jing LI, Zhijun GENG, Lugen ZUO. High expression of ATP5A1 in gastric carcinoma is correlated with a poor prognosis and enhanced glucose metabolism in tumor cells [J]. Journal of Southern Medical University, 2024, 44(5): 974-980. |
| [9] | SHEN Mengdi, ZHAO Na, DENG Xiaojing, DENG Min. High expression of COX6B2 in gastric cancer is associated with poor long-term prognosis and promotes cell proliferation and cell cycle progression by inhibiting p53 signaling [J]. Journal of Southern Medical University, 2024, 44(2): 289-297. |
| [10] | ZHANG Nuo, ZHANG Zhen, ZHANG Yulu, SONG Xue, ZHANG Xiaofeng, LI Jing, ZUO Lugen, HU Jianguo. PCID2 is highly expressed in gastric cancer and affects the prognosis by regulating cancer cell cycle and proliferation [J]. Journal of Southern Medical University, 2024, 44(2): 324-332. |
| [11] | ZHANG Wenjing, ZHANG Nuo, YANG Zi, ZHANG Xiaofeng, SUN Aofei, WANG Lian, SONG Xue, GENG Zhijun, LI Jing, HU Jianguo. Overexpression of BZW1 promotes invasion and metastasis of gastric cancer cells by regulating Wnt/β-catenin signaling and promoting epithelial-mesenchymal transition [J]. Journal of Southern Medical University, 2024, 44(2): 354-362. |
| [12] | Ruxue TAN, Xiaozhang BAO, Liang HAN, Zhaohui LI, Nan TIAN. A two-site combined prediction model based on HOXA9 DNA methylation for early screening of risks of meningioma progression [J]. Journal of Southern Medical University, 2024, 44(11): 2110-2120. |
| [13] | Zhen ZHANG, Hui LU, Xiaohua CHEN, Lian WANG, Ziliang WANG, Yueyue WANG, Sitang GE, Lugen ZUO. CEP192 overexpression is correlated with poor prognosis of gastric cancer and promotes gastric cancer cell proliferation by regulating PLK1/CDK1/Cyclin B1 signaling [J]. Journal of Southern Medical University, 2024, 44(11): 2137-2145. |
| [14] | DUAN Ting, ZHANG Zhen, SHI Jinran, XIAO Linyu, YANG Jingjing, YIN Lixia, ZHANG Xiaofeng, GENG Zhijun, LU Guoyu. High expression of CPNE3 correlates with poor long-term prognosis of gastric cancer by inhibiting cell apoptosis via activating PI3K/AKT signaling [J]. Journal of Southern Medical University, 2024, 44(1): 129-137. |
| [15] | YAO Yina, LIU Jia, ZHOU Xiangjun, LIU Zeyu, QIU Shizhen, HE Yingzheng, ZHOU Xueqiong. A pan-cancer analysis of TTC9A expression level and its correlation with prognosis and immune microenvironment [J]. Journal of Southern Medical University, 2024, 44(1): 70-82. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||