南方医科大学学报 ›› 2026, Vol. 46 ›› Issue (4): 761-769.doi: 10.12122/j.issn.1673-4254.2026.04.05
• • 上一篇
刘星扬1( ), 吴静涵1, 叶春艳1, 王锷1,2(), 胡浩1()
), 吴静涵1, 叶春艳1, 王锷1,2(), 胡浩1()
收稿日期:2025-11-22
出版日期:2026-04-20
发布日期:2026-04-24
通讯作者:
王锷,胡浩
E-mail:198112348@csu.edu.cn;ewang324@csu.edu.cn;mzwsq7413@163.com
作者简介:刘星扬,博士,E-mail: 198112348@csu.edu.cn
基金资助:
Xingyang LIU1(), Jinghan WU1, Chunyan YE1, E WANG1,2(), Hao HU1()
Received:2025-11-22
Online:2026-04-20
Published:2026-04-24
Contact:
E WANG, Hao HU
E-mail:198112348@csu.edu.cn;ewang324@csu.edu.cn;mzwsq7413@163.com
Supported by:摘要:
目的 颈动脉血流减少与围术期脑血管及神经系统并发症密切相关,但其在全身麻醉期间的变化规律及生理调控因素仍缺乏系统认识。 方法 前瞻性纳入193例接受腹部手术的老年患者,连续记录围术期呼吸、循环参数及麻醉深度指标。采用矢量血流成像技术在多个关键时间点测量颈总动脉(CCA)血流量。将心率、平均动脉压、呼气末二氧化碳及双频指数纳入线性混合效应模型,并以患者作为随机效应,分析并解释术中CCA血流变化的生理决定因素。 结果 老年患者在全身麻醉期间CCA血流呈现明显的阶段性波动。线性混合效应模型可解释术中CCA血流变异的52.0%(调整后R²=0.520,P<0.001)。心率、平均动脉压、呼气末二氧化碳及双频指数均与颈动脉血流变化显著相关(P<0.001)。标准化模型进一步显示,不同生理指标对CCA血流的调节强度存在明显差异,其中血流动力学相关指标的影响高于血压或心率变化。手术方式及手术体位对颈动脉血流无显著影响。 结论 本研究从整体生理调控角度表明,术中脑灌注并非单纯依赖血压维持,而是受到通气水平、循环状态及麻醉深度的协同调控。有效识别和管理相关影响因素有助于优化术中脑灌注。
刘星扬, 吴静涵, 叶春艳, 王锷, 胡浩. 老年患者全麻期间颈总动脉血流的动态变化及其生理调控机制:一项前瞻性研究[J]. 南方医科大学学报, 2026, 46(4): 761-769.
Xingyang LIU, Jinghan WU, Chunyan YE, E WANG, Hao HU. Dynamic changes and physiological regulation of common carotid artery blood flow during general anesthesia in elderly patients: a prospective study[J]. Journal of Southern Medical University, 2026, 46(4): 761-769.
| Variable | Parameter |
|---|---|
| Age (year) | 69.28±3.71 |
| Male [n (%)] | 102.00 (52.85) |
| BMI (kg/m2) | 22.64±2.99 |
| ASA physical status [n (%)] | |
| II | 62.00 (32.12) |
| III | 131.00 (67.88) |
| Complication [n (%)] | |
| Hypertension | 77.00 (39.90) |
| Diabetes | 31.00 (16.06) |
| Coronary heart disease | 12.00 (6.22) |
| Smoking history [n (%)] | 64.00 (33.16) |
| Alcohol use history [n (%)] | 48.00 (24.87) |
| Operative site [n (%)] | |
| Stomach | 47.00 (24.35) |
| Colon | 86.00 (44.56) |
| Rectal | 48.00 (24.87) |
| Other | 12.00 (6.22) |
| Operative approachs [n (%)] | |
| Laparotomy | 35.00 (18.13) |
| Laparoscopy | 158.00 (81.87) |
表1 受试者基线特征
Tab.1 Baseline characteristics of the enrolled patients (n=193)
| Variable | Parameter |
|---|---|
| Age (year) | 69.28±3.71 |
| Male [n (%)] | 102.00 (52.85) |
| BMI (kg/m2) | 22.64±2.99 |
| ASA physical status [n (%)] | |
| II | 62.00 (32.12) |
| III | 131.00 (67.88) |
| Complication [n (%)] | |
| Hypertension | 77.00 (39.90) |
| Diabetes | 31.00 (16.06) |
| Coronary heart disease | 12.00 (6.22) |
| Smoking history [n (%)] | 64.00 (33.16) |
| Alcohol use history [n (%)] | 48.00 (24.87) |
| Operative site [n (%)] | |
| Stomach | 47.00 (24.35) |
| Colon | 86.00 (44.56) |
| Rectal | 48.00 (24.87) |
| Other | 12.00 (6.22) |
| Operative approachs [n (%)] | |
| Laparotomy | 35.00 (18.13) |
| Laparoscopy | 158.00 (81.87) |
| Variable | Awake (T1) | After induction of anaesthesia (T2) | 5 min after surgery started (T3) | At the end of the surgery (T4) |
|---|---|---|---|---|
| CCA blood flow (mL/min) a | 319.45 (274.66-367.55) | 242.10 (195.05-306.30) | 228.90 (175.10-301.55) | 224.80 (179.45-276.80) |
| CCA PSV (cm/s)b | 55.02±10.15 | 51.03±11.01 | 44.59±10.52 | 45.17±9.43 |
| MAP (mmHg)b | 92.44±15.35 | 79.76±14.54 | 89.20±10.93 | 82.97±9.28 |
| SBP (mmHg)b | 136.53±18.19 | 116.32±22.67 | 129.74±17.10 | 124.19±14.58 |
| HR (beat/min)a | 73.00 (67.00-81.00) | 62.00 (57.50-68.00) | 61.00 (56.00-67.00) | 59.00 (55.00-64.00) |
| BISa | 95.00 (93.00-97.00) | 47.00 (42.00-53.00) | 42.00 (39.00-46.00) | 48.00 (44.00-52.0) |
| ETCO2 (mmHg)b | 30.48±5.21c | 33.73±3.81 | 34.18±4.09 | 32.55±4.02 |
表2 围术期颈总动脉(CCA)血流及常规监测指标的变化
Tab.2 Changes in perioperative common carotid artery (CCA) blood flow and routine monitoring indicators (n=193)
| Variable | Awake (T1) | After induction of anaesthesia (T2) | 5 min after surgery started (T3) | At the end of the surgery (T4) |
|---|---|---|---|---|
| CCA blood flow (mL/min) a | 319.45 (274.66-367.55) | 242.10 (195.05-306.30) | 228.90 (175.10-301.55) | 224.80 (179.45-276.80) |
| CCA PSV (cm/s)b | 55.02±10.15 | 51.03±11.01 | 44.59±10.52 | 45.17±9.43 |
| MAP (mmHg)b | 92.44±15.35 | 79.76±14.54 | 89.20±10.93 | 82.97±9.28 |
| SBP (mmHg)b | 136.53±18.19 | 116.32±22.67 | 129.74±17.10 | 124.19±14.58 |
| HR (beat/min)a | 73.00 (67.00-81.00) | 62.00 (57.50-68.00) | 61.00 (56.00-67.00) | 59.00 (55.00-64.00) |
| BISa | 95.00 (93.00-97.00) | 47.00 (42.00-53.00) | 42.00 (39.00-46.00) | 48.00 (44.00-52.0) |
| ETCO2 (mmHg)b | 30.48±5.21c | 33.73±3.81 | 34.18±4.09 | 32.55±4.02 |
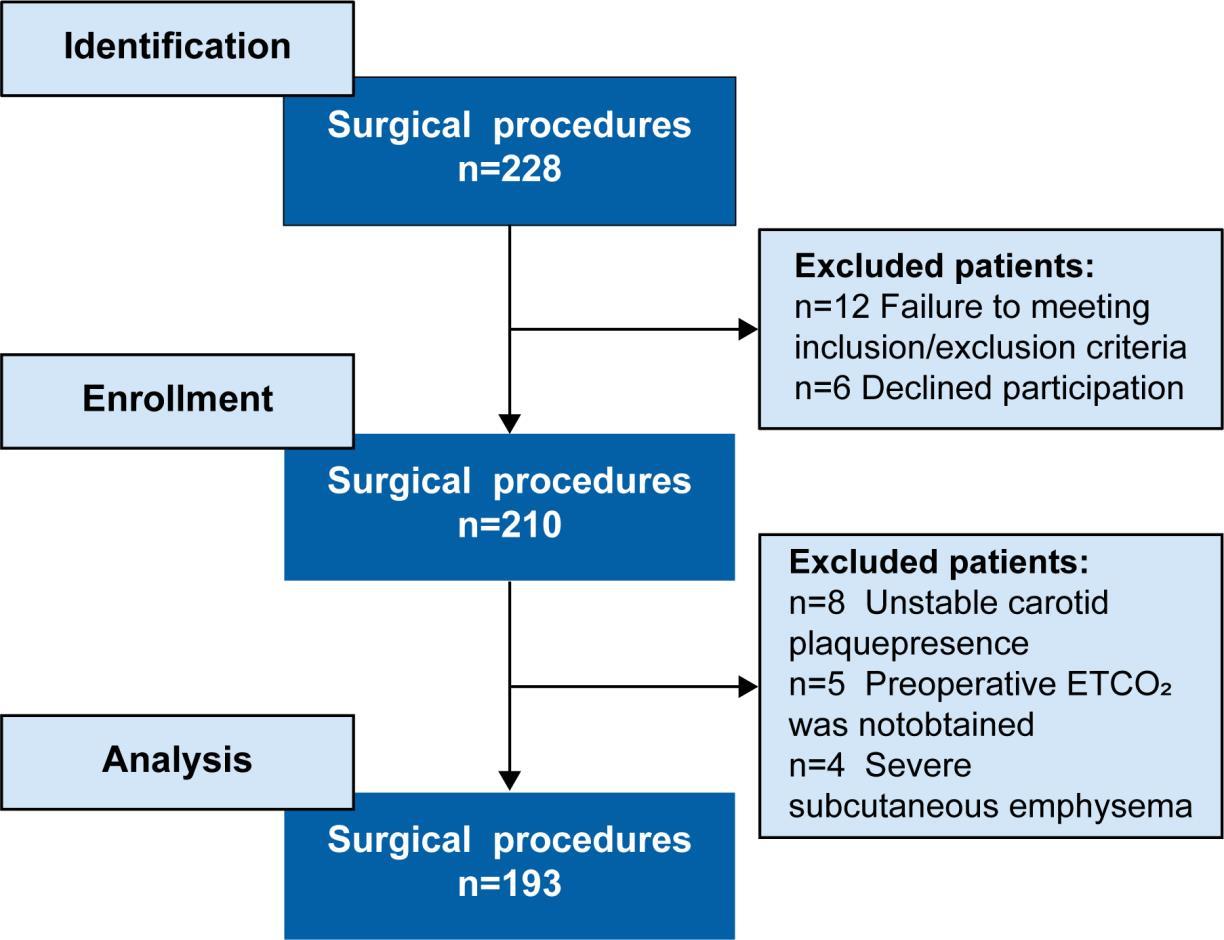
图1 流程图
Fig.1 Flow chart of patient enrollment. ETCO2: End-tidal carbon dioxide.
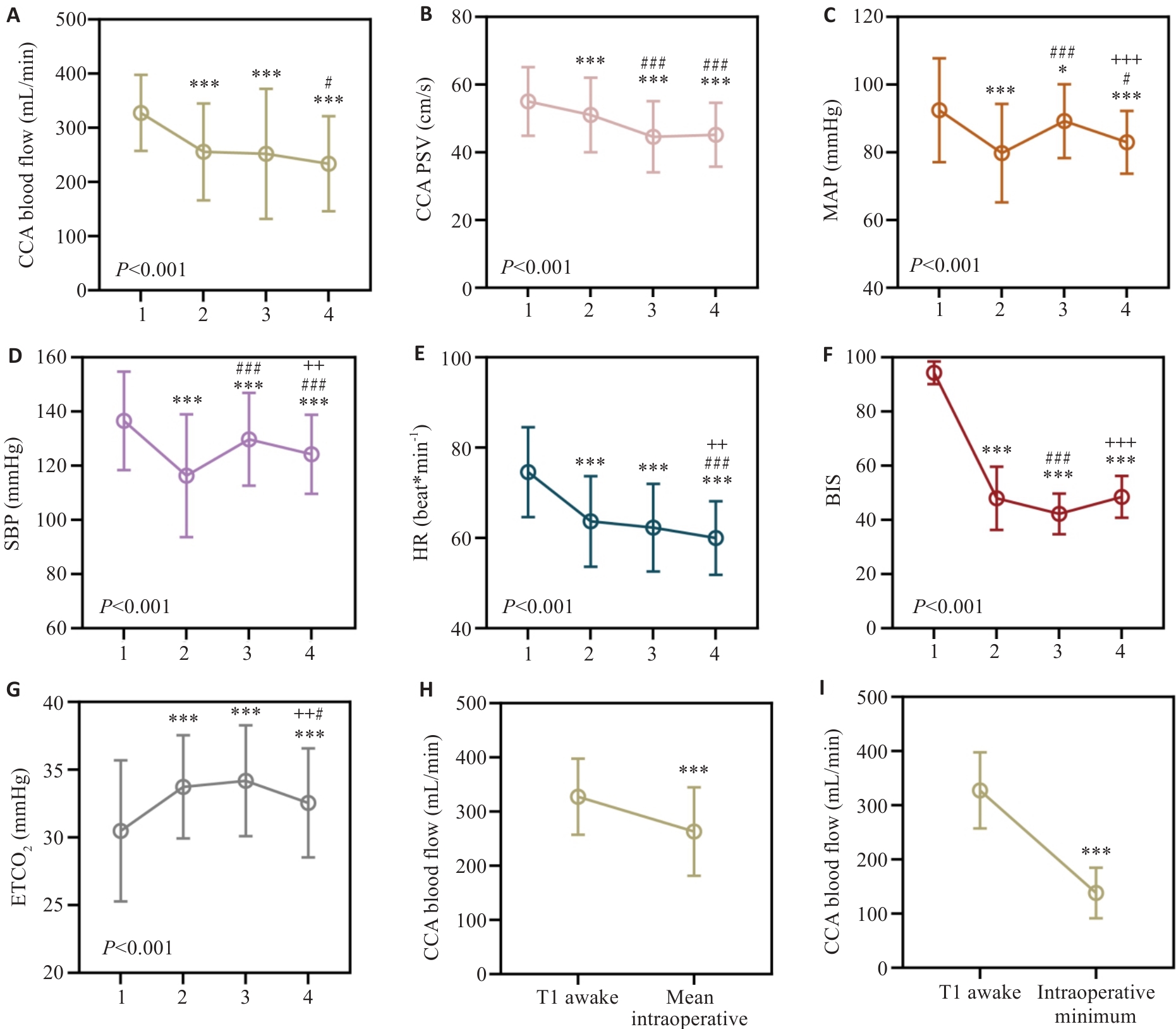
图2 围术期颈总动脉(CCA)血流及常规监测指标的变化
Fig.2 Perioperative changes in CCA blood flow and routine monitoring indicators (n=193). A: CCA blood flow; B: Peak systolic velocity (PSV); C: Mean arterial pressure (MAP); D: Systolic blood pressure (SBP); E: Heart rate (HR); F: Bispectral index (BIS); G: End-tidal carbon dioxide (ETCO2). All variables were measured at awake supine state (T1), 5 min after induction of anesthesia (T2), 5 min after the start of surgery (T3), and at the end of surgery(T4). H: Change in CCA blood flow between the awake state (T1) and the intraoperative mean value. The intraoperative mean CCA blood flow was calculated as the average of measurements taken every 10 min during surgery. I: Change in CCA blood flow between the awake state (T1) and the intraoperative minimum value. In A-G, the overall time effect was assessed using repeated-measures ANOVA, and the corresponding P value was presented in the lower left corner of each figure. Pairwise comparisons between time points were conducted within the same analytical framework using Tukey's adjustment for multiple comparisons. *P<0.05, ***P<0.001 vs T1; #P<0.05, ###P<0.001 vs T2; ++P<0.01, +++P<0.001 vs T3. In H and I.
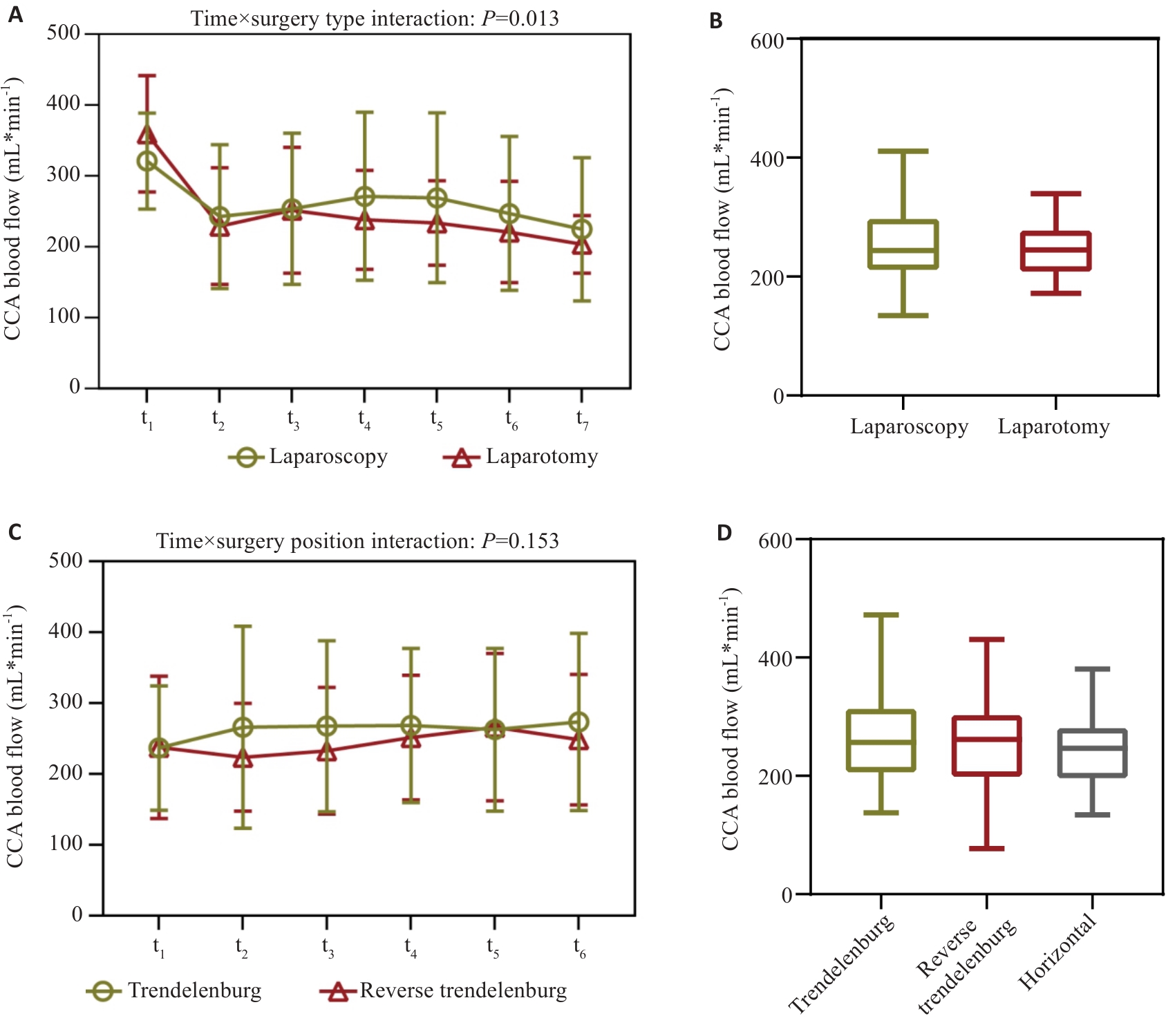
图3 不同手术方式及体位下术中多个时间点的CCA血流变化
Fig.3 Changes in intraoperative CCA blood flow at multiple time points under different surgical approaches and patient positions. A, B: Operative approaches included laparoscopy (n=158) and laparotomy (n=35). The time points recorded were as follows: (t1) preoperative awake state; (t2) 5 min after surgery started; (t3) 30 min after surgery started; (t4) 60 min after surgery started; (t5) 90 min after surgery started; (t6) 120 min after surgery started; and (t7) at the end of the surgery. C, D: Operation position included Trendelenburg (n=110), reverse Trendelenburg (n=48), and horizontal (n=35). The time points recorded were as follows: (t1) before the change in position; (t2) 5 min after the postural change; (t3) 10 min after the postural change; (t4) 20 min after the postural change; (t5) 30 min after the postural change; and (t6) 60 min after the postural change.
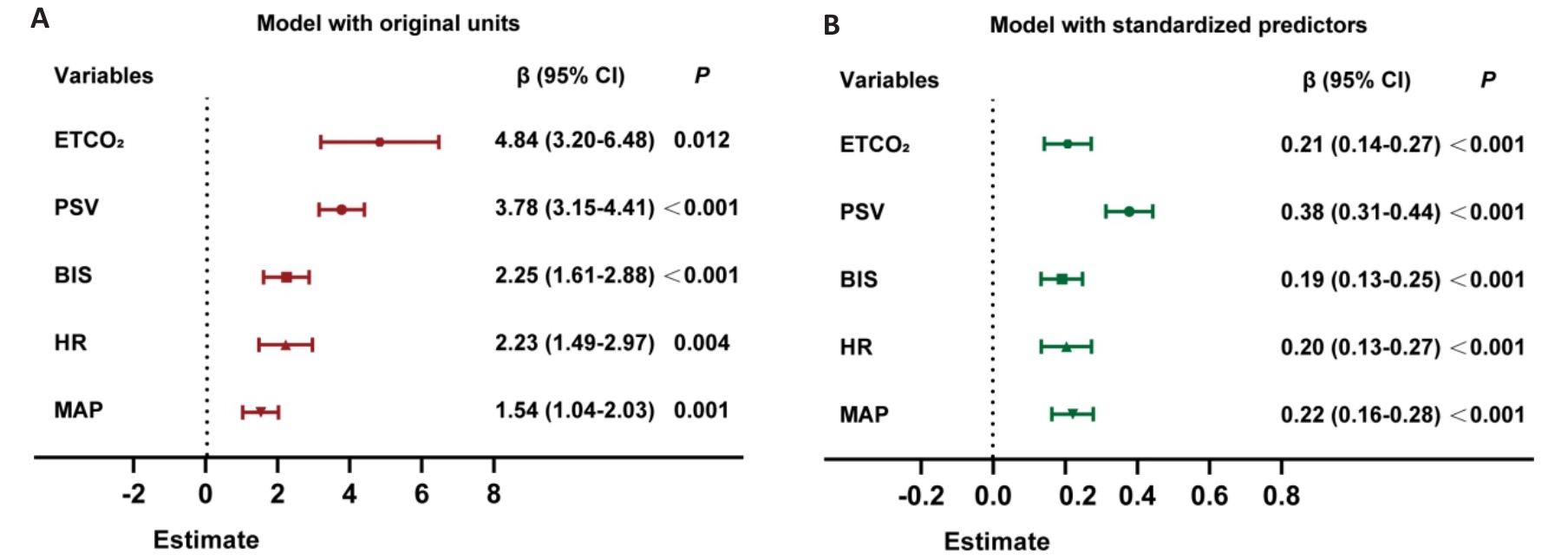
图4 混合线性模型森林图: 不同生理指标对CCA血流的影响
Fig.4 Forest plots of the linear mixed-effects models showing the effects of physiological variables on CCA blood flow. A: Model constructed using original measurement scales, illustrating the change in CCA blood flow per unit increase of each variable. B: Model constructed with Z-score-standardized predictors, allowing comparison of the relative strength of effects among variables. Data from 193 patients at 3 intraoperative time points were included (T2: after induction of anesthesia; T3: 5 min after surgery started; T4: at the end of surgery).
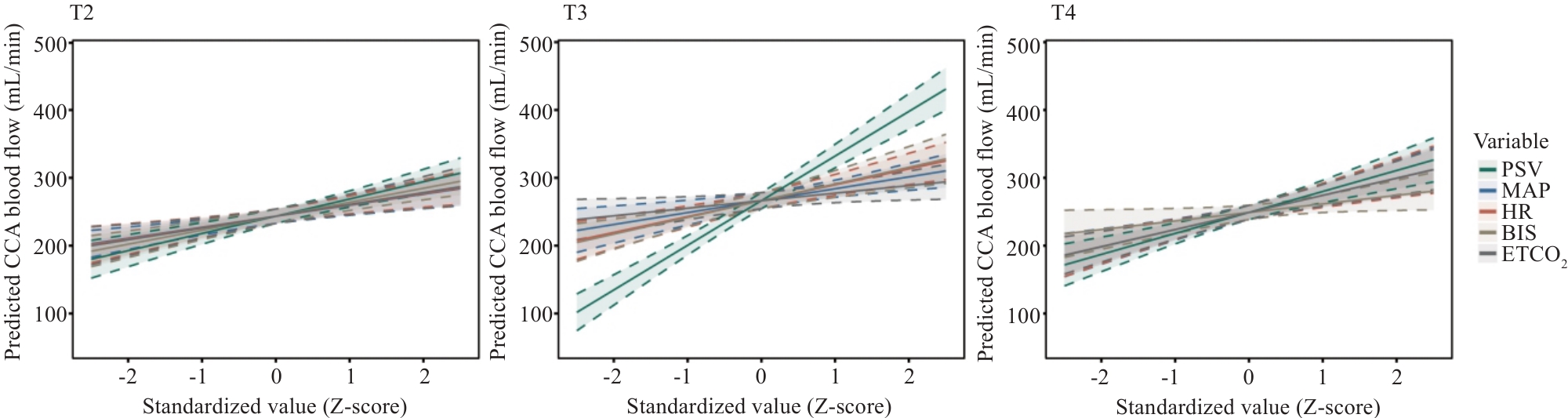
图5 不同手术阶段各生理指标对CCA血流影响的混合效应模型预测曲线
Fig.5 Changes in intraoperative CCA blood flow at multiple time points under different surgical approaches and patient positions. The x-axis shows standardized values (Z-scores) of physiological variables, and the y-axis shows predicted CCA blood flow. Shaded areas represent 95% confidence intervals, with dashed lines indicating the boundaries. Only PSV shows a visibly reduced slope during surgical initiation (T3), which returns to a pattern similar to T2 and T4, indicating a phase-specific effect of PSV on carotid blood flow. Other variables show nearly parallel slopes across phases, suggesting no significant interaction with time.
| Variable | β | 95% CI | P |
|---|---|---|---|
| PSV | -2.867 | -3.80 to -1.93 | <0.001 |
| MAP | 0.206 | -0.60 to 1.01 | 0.618 |
| HR | -0.212 | -1.24 to 0.82 | 0.685 |
| BIS | -0.686 | -1.84 to 0.47 | 0.244 |
| ETCO2 | 2.076 | -0.35 to 4.50 | 0.094 |
表3 各生理指标与手术阶段(T3)交互项的线性混合效应模型结果
Tab.3 Interaction terms between physiological variables and surgical phase (T3) in the mixed-effects model
| Variable | β | 95% CI | P |
|---|---|---|---|
| PSV | -2.867 | -3.80 to -1.93 | <0.001 |
| MAP | 0.206 | -0.60 to 1.01 | 0.618 |
| HR | -0.212 | -1.24 to 0.82 | 0.685 |
| BIS | -0.686 | -1.84 to 0.47 | 0.244 |
| ETCO2 | 2.076 | -0.35 to 4.50 | 0.094 |
| [1] | Bird CM. The role of the hippocampus in recognition memory[J]. Cortex, 2017, 93: 155-65. doi:10.1016/j.cortex.2017.05.016 |
| [2] | Bown CW, Do R, Khan OA, et al. Lower cardiac output relates to longitudinal cognitive decline in aging adults[J]. Front Psychol, 2020, 11: 569355. doi:10.3389/fpsyg.2020.569355 |
| [3] | Slupe AM, Kirsch JR. Effects of anesthesia on cerebral blood flow, metabolism, and neuroprotection[J]. J Cereb Blood Flow Metab, 2018, 38(12): 2192-208. doi:10.1177/0271678x18789273 |
| [4] | Mrkobrada M, Chan MTV, Cowan D, et al. Perioperative covert stroke in patients undergoing non-cardiac surgery (NeuroVISION): a prospective cohort study[J]. Lancet, 2019, 394(10203): 1022-9. doi:10.1016/s0140-6736(19)31795-7 |
| [5] | Mrkobrada M, Hill MD, Chan MTV, et al. Covert stroke after non-cardiac surgery: a prospective cohort study[J]. Br J Anaesth, 2016, 117(2): 191-7. doi:10.1093/bja/aew179 |
| [6] | Tzeng YC, Panerai RB. CrossTalk proposal: dynamic cerebral autoregulation should be quantified using spontaneous blood pressure fluctuations[J]. J Physiol, 2018, 596(1): 3-5. doi:10.1113/JP273899 |
| [7] | Barnes SC, Panerai RB, Beishon L, et al. Cerebrovascular responses to somatomotor stimulation in Parkinson's disease: a multivariate analysis[J]. J Cereb Blood Flow Metab, 2022, 42(8): 1547-58. doi:10.1177/0271678X211065204 |
| [8] | Cai JH, Tang M, Wu HY, et al. Association of intraoperative hypotension and severe postoperative complications during non-cardiac surgery in adult patients: a systematic review and meta-analysis[J]. Heliyon, 2023, 9(5): e15997. doi:10.1016/j.heliyon.2023.e15997 |
| [9] | Zarour S, Weiss Y, Abu-Ghanim M, et al. Association between intraoperative hypotension and postoperative delirium: a retro-spective cohort analysis[J]. Anesthesiology, 2024, 141(4): 707-18. doi:10.1097/aln.0000000000005149 |
| [10] | Ghosh A, Elwell C, Smith M. Cerebral near-infrared spectroscopy in adults: a work in progress[J]. Anesth & Analg, 2012, 115(6): 1373-83. doi:10.1213/ane.0b013e31826dd6a6 |
| [11] | Bonow RH, Young CC, Bass DI, et al. Transcranial Doppler ultrasonography in neurological surgery and neurocritical care[J]. Neurosurg Focus, 2019, 47(6): E2. doi:10.3171/2019.9.focus19611 |
| [12] | Demir I, Turktan M, Gulec E, et al. The predictive role of carotid artery flow time for anesthesia-induced hypotension in high-risk elderly patients[J]. J Clin Monit Comput, 2024, 38(4): 859-67. doi:10.1007/s10877-024-01145-2 |
| [13] | Skytioti M, Elstad M, Søvik S. Internal carotid artery blood flow response to anesthesia, pneumoperitoneum, and head-up tilt during laparoscopic cholecystectomy[J]. Anesthesiology, 2019, 131(3): 512-20. doi:10.1097/ALN.0000000000002838 |
| [14] | Oncu K and Saylan S, Effects of Haemodynamic Changes Caused by Different Pneumoperitoneum Pressures on Cerebral Oxygenation in Laparoscopic Cholecystectomy: Prospective Randomised Controlled Trial[J]. J Coll Physicians Surg Pak, 2024. 34(1): 16-21. doi:10.29271/jcpsp.2024.01.16 |
| [15] | Boyajian RA, Schwend RB, Wolfe MM, et al. Measurement of anterior and posterior circulation flow contributions to cerebral blood flow[J]. J Neuroimaging, 1995, 5(1): 1-3. doi:10.1111/jon1995511 |
| [16] | Brandt AH, Olesen JB, Moshavegh R, et al. Common carotid artery volume flow: a comparison study between ultrasound vector flow imaging and phase contrast magnetic resonance imaging[J]. Neurol Int, 2021, 13(3): 269-78. doi:10.3390/neurolint13030028 |
| [17] | Sun L, Wu G, Zhou Y, et al. Prospective study on ultrasound-guided stellate ganglion block improves cerebral blood flow in patients with stroke[J]. J Stroke Cerebrovasc Dis, 2024, 33(4): 107593. doi:10.1016/j.jstrokecerebrovasdis.2024.107593 |
| [18] | Yu FX, Liu D, Ma X, et al. Dobutamine-induced alterations in internal carotid artery blood flow and cerebral blood flow in healthy adults[J]. Brain Res Bull, 2025, 221: 111204. doi:10.1016/j.brainresbull.2025.111204 |
| [19] | Kang H. Sample size determination and power analysis using the G*Power software[J]. J Educ Eval Health Prof, 2021, 18: 17. doi:10.3352/jeehp.2021.18.17 |
| [20] | Bai CH, Chen JR, Chiu HC, et al. Lower blood flow velocity, higher resistance index, and larger diameter of extracranial carotid arteries are associated with ischemic stroke independently of carotid athero-sclerosis and cardiovascular risk factors[J]. J Clin Ultrasound, 2007, 35(6): 322-30. doi:10.1002/jcu.20351 |
| [21] | Kure CE, Rosenfeldt FL, Scholey AB, et al. Relationships among cognitive function and cerebral blood flow, oxidative stress, and inflammation in older heart failure patients[J]. J Card Fail, 2016, 22(7): 548-59. doi:10.1016/j.cardfail.2016.03.006 |
| [22] | Bernardi MH, Wahrmann M, Dworschak M, et al. Carotid artery blood flow velocities during open-heart surgery and its association with delirium: a prospective, observational pilot study[J]. Medicine, 2019, 98(50): e18234. doi:10.1097/MD.0000000000018234 |
| [23] | Xu N, Li LX, Wang TL, et al. Processed multiparameter electroencephalogram-guided general anesthesia management can reduce postoperative delirium following carotid endarterectomy: a randomized clinical trial[J]. Front Neurol, 2021, 12: 666814. doi:10.3389/fneur.2021.666814 |
| [24] | Lopez MG, Pandharipande P, Morse J, et al. Intraoperative cerebral oxygenation, oxidative injury, and delirium following cardiac surgery[J]. Free Radic Biol Med, 2017, 103: 192-8. doi:10.1016/j.freeradbiomed.2016.12.039 |
| [25] | Zhao Y, Zhang JW, Zheng YL, et al. NAD(+) improves cognitive function and reduces neuroinflammation by ameliorating mitochondrial damage and decreasing ROS production in chronic cerebral hypoperfusion models through Sirt1/PGC-1α pathway[J]. J Neuroinflammation, 2021, 18(1): 207. doi:10.1186/s12974-021-02250-8 |
| [26] | Shibata M, Ohtani R, Ihara M, et al. White matter lesions and glial activation in a novel mouse model of chronic cerebral hypoperfusion[J]. Stroke, 2004, 35(11): 2598-603. doi:10.1161/01.str.0000143725.19053.60 |
| [27] | Swarbrick CJ, Partridge JSL. Evidence-based strategies to reduce the incidence of postoperative delirium: a narrative review[J]. Anaesthesia, 2022, 77(S1): 92-101. doi:10.1111/anae.15607 |
| [28] | Pereira EM, Moraes VR, Gaya da Costa M, et al. Remimazolam vs. propofol for general anaesthesia in elderly patients: a meta-analysis with trial sequential analysis[J]. Eur J Anaesthesiol, 2024, 41(10): 738-48. doi:10.1097/01.EJA.0001179540.00282.be |
| [29] | Tzeng YC, Ainslie PN. Blood pressure regulation IX: cerebral autoregulation under blood pressure challenges[J]. Eur J Appl Physiol, 2014, 114(3): 545-59. doi:10.1007/s00421-013-2667-y |
| [30] | Son JS, Oh JY, Ko S. Effects of hypercapnia on postoperative nausea and vomiting after laparoscopic surgery: a double-blind randomized controlled study[J]. Surg Endosc, 2017, 31(11): 4576-82. doi:10.1007/s00464-017-5519-8 |
| [31] | Gordon GR. Neurovascular coupling during hypercapnia in cerebral blood flow regulation[J]. Nat Commun, 2024, 15: 7636. doi:10.1038/s41467-024-50165-8 |
| [32] | Willie CK, MacLeod DB, Shaw AD, et al. Regional brain blood flow in man during acute changes in arterial blood gases[J]. J Physiol, 2012, 590(14): 3261-75. doi:10.1113/jphysiol.2012.228551 |
| [33] | Claassen JAHR, Thijssen DHJ, Panerai RB, et al. Regulation of cerebral blood flow in humans: physiology and clinical implications of autoregulation[J]. Physiol Rev, 2021, 101(4): 1487-559. doi:10.1152/physrev.00022.2020 |
| [34] | Au JS, Yiu BYS, So H, et al. Ultrasound vector projectile imaging for detection of altered carotid bifurcation hemodynamics during reductions in cardiac output[J]. Med Phys, 2020, 47(2): 431-40. doi:10.1002/mp.13905 |
| [35] | Qiu YJ, Yang DH, Zhang Q, et al. V Flow technology in measurement of wall shear stress of common carotid arteries in healthy adults: Feasibility and normal values[J]. Clin Hemorheol Microcirc, 2020, 74(4): 453-62. doi:10.3233/ch-190719 |
| [36] | Song D, Liu MM, Dong YH, et al. Investigation on the differences of hemodynamics in normal common carotid, subclavian, and common femoral arteries using the vector flow technique[J]. Front Cardiovasc Med, 2022, 9: 956023. doi:10.3389/fcvm.2022.956023 |
| [37] | Du YG, Ding HY, He L, et al. Quantitative blood flow measurements in the common carotid artery: a comparative study of high-frame-rate ultrasound vector flow imaging, pulsed wave Doppler, and phase contrast magnetic resonance imaging[J]. Diagnostics, 2022, 12(3): 690. doi:10.3390/diagnostics12030690 |
| [38] | Poloni S, Bozzetto M, Du YG, et al. Velocity vector comparison between vector flow imaging and computational fluid dynamics in the carotid bifurcation[J]. Ultrasonics, 2023, 128: 106860. doi:10.1016/j.ultras.2022.106860 |
| [39] | Brandt AH, Hansen KL, Ewertsen C, et al. A comparison study of vector velocity, spectral Doppler and magnetic resonance of blood flow in the common carotid artery[J]. Ultrasound Med Biol, 2018, 44(8): 1751-61. doi:10.1016/j.ultrasmedbio.2018.05.002 |
| [1] | 吕雪彩, 刘艳红, 韩诗怡, 张浩赟, 侯爱生, 周志康, 史立凯, 高洁, 曹江北, 张宏, 米卫东. 老年患者胃肠道手术后综合并发症的危险因素——一项多中心观察性研究[J]. 南方医科大学学报, 2025, 45(4): 736-743. |
| [2] | 原梦瑶, 阮湘涵, 李扬, 张婷, 郝春香, 李皓, 娄景盛, 曹江北, 刘艳红, 米卫东, 张晓莹. 术前血清镁水平与非心脏手术老年患者术后谵妄风险的关系:一项回顾性队列研究[J]. 南方医科大学学报, 2025, 45(12): 2616-2627. |
| [3] | 冯青波, 骆春梅, 刘向红, 许 婷, 杜 芹. 全麻与深度镇静下的儿童口腔治疗:家长接受度、口腔健康相关生活质量及疗效是否有差异?[J]. 南方医科大学学报, 2023, 43(4): 604-610. |
| [4] | 牛善洲, 刘 宏, 刘沛沄, 张梦真, 李 硕, 梁礼境, 李 楠, 刘国良. 基于非局部低秩稀疏矩阵分解的低剂量脑灌注CT图像恢复方法[J]. 南方医科大学学报, 2022, 42(9): 1309-1316. |
| [5] | 许立倩, 魏 宁, 单美娟, 汪子怡, 叶天成, 梁赛珍, 李 乐, 朱 强, 何路遥, 白建杰, 陈碧霞, 徐金东. 加温湿化高流量鼻导管吸氧可减少老年患者麻醉复苏期缺氧事件发生[J]. 南方医科大学学报, 2021, 41(8): 1265-1269. |
| [6] | 牛善洲, 刘 宏, 刘沛沄, 张梦真, 邱 洋, 黎 钰, 谢国强, 刘国良, 卢绍辉. 低剂量脑灌注CT图像恢复方法:基于先验图像约束扩散张量[J]. 南方医科大学学报, 2021, 41(8): 1226-1233. |
| [7] | 陈小慧,任晓强,马亚兵,葛莉,胡钟元,阎文军. 术后疼痛引起老年患者术后认知功能障碍的相关机制研究进展[J]. 南方医科大学学报, 2019, 39(09): 1122-. |
| [8] | 李子嘉,芦坤,王凯,赵颖茵,黄霞,靳三庆. 全麻诱导期间空气面罩通气与纯氧面罩通气的无通气安全时限和气管插管时长的比较[J]. 南方医科大学学报, 2017, 37(12): 1643-. |
| [9] | 田秀梅,黄静,林嘉慧,张忻宇,马建华,边兆英. 投影数据恢复方法在低剂量脑灌注CT成像中的应用[J]. 南方医科大学学报, 2017, 37(04): 470-. |
| [10] | 吴涯雯,黄鸿晖,曾静贤,李步龙,雷学恒,陈友权. 右美托咪啶用于妇科腹腔镜手术全麻后寒战的效果:前瞻性、随机、单盲、临床对比研究[J]. 南方医科大学学报, 2013, 33(04): 611-. |
| [11] | 孙长江,张西志,陈勇. 厄洛替尼治疗老年晚期非小细胞肺癌的疗效[J]. 南方医科大学学报, 2012, 32(12): 1839-. |
| [12] | 黄劲松,黄克力,简旭华,吴敏,卢聪,郑少忆. 50岁以上的主动脉瓣病变患者的外科治疗:附73例报告[J]. 南方医科大学学报, 2012, 32(02): 258-. |
| [13] | 李申一; 雷毅; 徐世元; 王晓军; 赵涛; 赵华; 彭铖; 李杉;. 悬雍垂腭咽成型术的麻醉处理(附786例报告)[J]. 南方医科大学学报, 2006, 26(11): 1673-1674. |
| [14] | 王刚; 张双全; 詹鸿;. 石杉碱甲对老年患者全麻苏醒期脑内胆碱酯酶和乙酰胆碱的影响[J]. 南方医科大学学报, 2006, 26(11): 1660-1662. |
| [15] | 高勇; 邹小明; 王武军; 刘高望; 古妙宁;. 深低温停循环中不同脑灌注方式脑保护的实验研究[J]. 南方医科大学学报, 2006, 26(05): 644-647. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||