Journal of Southern Medical University ›› 2026, Vol. 46 ›› Issue (1): 159-165.doi: 10.12122/j.issn.1673-4254.2026.01.17
Previous Articles Next Articles
Xiyu GAO( ), Jing XIAO, Na FENG, Chen GUO, Lifei CAO, Chunyan ZHANG, Yan ZHANG, Tuo HAN()
), Jing XIAO, Na FENG, Chen GUO, Lifei CAO, Chunyan ZHANG, Yan ZHANG, Tuo HAN()
Received:2025-07-10
Online:2026-01-20
Published:2026-01-16
Contact:
Tuo HAN
E-mail:eclipse070@stu.xjtu.edu.cn;heart0228@xjtu.edu.cn
Supported by:Xiyu GAO, Jing XIAO, Na FENG, Chen GUO, Lifei CAO, Chunyan ZHANG, Yan ZHANG, Tuo HAN. β‑blockers after percutaneous coronary intervention does not reduce risks of all-cause mortality or major adverse cardiovascular events in patients with stable coronary artery disease[J]. Journal of Southern Medical University, 2026, 46(1): 159-165.
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.j-smu.com/EN/10.12122/j.issn.1673-4254.2026.01.17
| Variable | Total (n=204) | Control group (n=149) | β-blocker group (n=55) | Statistic | P |
|---|---|---|---|---|---|
| Age (year) | 72.6±10.3 | 72.9±10.1 | 71.8±11.0 | 0.416 | 0.520 |
| Gender [n (%)] | 0.060 | 0.806 | |||
| Female | 62 (30.4) | 46 (30.9) | 16 (29.1) | ||
| Male | 142 (69.6) | 103 (69.1) | 39 (70.9) | ||
| Smoking [n (%)] | 101 (49.5) | 77 (51.7) | 24 (43.6) | 1.039 | 0.308 |
| BMI (kg/m2) | 23.6±3.9 | 23.4±3.8 | 24.3±4.1 | 2.018 | 0.157 |
| SBP (mmHg) | 136.3±20.4 | 135.8±19.6 | 137.5±22.7 | 0.254 | 0.615 |
| DBP (mmHg) | 77.4±13.2 | 77.2±12.9 | 77.9±14.1 | 0.108 | 0.743 |
| Hemoglobin (g/dL) | 13.6±2.0 | 13.6±1.9 | 13.5±2.2 | 0.037 | 0.847 |
| Albumin (g/L) | 3.9±0.5 | 3.9±0.5 | 3.9±0.5 | 0.167 | 0.683 |
| eGFR (mL/min/1.73 m2) | 61.3±24.6 | 63.8±24.2 | 54.7±24.6 | 5.583 | 0.019 |
| AST (U/L) | 24.7±11.0 | 25.5±11.6 | 22.6±8.7 | 2.841 | 0.093 |
| ALT (U/L) | 20.9±12.2 | 21.5±12.7 | 19.5±10.6 | 1.016 | 0.315 |
| TC (mg/dL) | 185.4±35.7 | 184.4±35.2 | 188.4±37.4 | 0.390 | 0.533 |
| TG (mg/dL) | 117.0 (83.5, 159.5) | 118.0 (84.0, 157.0) | 105.5 (73.5, 159.8) | 1.052 | 0.305 |
| HDL-C (mg/dL) | 50.2±13.2 | 49.9±13.0 | 51.1±13.8 | 0.314 | 0.576 |
| LDL-C (mg/dL) | 110.1±28.5 | 109.3±28.3 | 112.1±29.4 | 0.394 | 0.531 |
| HbA1C (%) | 6.0 (5.7, 6.7) | 6.0 (5.6, 6.6) | 6.0 (5.7, 7.0) | 2.139 | 0.144 |
| CRP (mg/dL) | 0.1 (0.0, 0.3) | 0.1 (0.0, 0.3) | 0.1 (0.1, 0.3) | 1.240 | 0.266 |
| LVEF (%) | 63.2±9.8 | 65.0±7.3 | 58.6±13.6 | 18.205 | <0.001 |
| Cerebral infarction [n (%)] | 35 (17.2) | 27 (18.1) | 8 (14.5) | 0.361 | 0.548 |
| Peripheral arterial disease [n (%)] | 53 (26.0) | 42 (28.2) | 11 (20) | 1.400 | 0.237 |
| Atrial fibrillation [n (%)] | 26 (12.7) | 13 (8.7) | 13 (23.6) | 8.032 | 0.005 |
| Hypertension [n (%)] | 151 (74.0) | 111 (74.5) | 40 (72.7) | 0.065 | 0.798 |
| Dyslipidemia [n (%)] | 104 (51.0) | 78 (52.3) | 26 (47.3) | 0.414 | 0.520 |
| Diabetes [n (%)] | 73 (35.8) | 50 (33.6) | 23 (41.8) | 1.193 | 0.275 |
Tab.1 Comparison of baseline characteristics between the β blocker users and non-users
| Variable | Total (n=204) | Control group (n=149) | β-blocker group (n=55) | Statistic | P |
|---|---|---|---|---|---|
| Age (year) | 72.6±10.3 | 72.9±10.1 | 71.8±11.0 | 0.416 | 0.520 |
| Gender [n (%)] | 0.060 | 0.806 | |||
| Female | 62 (30.4) | 46 (30.9) | 16 (29.1) | ||
| Male | 142 (69.6) | 103 (69.1) | 39 (70.9) | ||
| Smoking [n (%)] | 101 (49.5) | 77 (51.7) | 24 (43.6) | 1.039 | 0.308 |
| BMI (kg/m2) | 23.6±3.9 | 23.4±3.8 | 24.3±4.1 | 2.018 | 0.157 |
| SBP (mmHg) | 136.3±20.4 | 135.8±19.6 | 137.5±22.7 | 0.254 | 0.615 |
| DBP (mmHg) | 77.4±13.2 | 77.2±12.9 | 77.9±14.1 | 0.108 | 0.743 |
| Hemoglobin (g/dL) | 13.6±2.0 | 13.6±1.9 | 13.5±2.2 | 0.037 | 0.847 |
| Albumin (g/L) | 3.9±0.5 | 3.9±0.5 | 3.9±0.5 | 0.167 | 0.683 |
| eGFR (mL/min/1.73 m2) | 61.3±24.6 | 63.8±24.2 | 54.7±24.6 | 5.583 | 0.019 |
| AST (U/L) | 24.7±11.0 | 25.5±11.6 | 22.6±8.7 | 2.841 | 0.093 |
| ALT (U/L) | 20.9±12.2 | 21.5±12.7 | 19.5±10.6 | 1.016 | 0.315 |
| TC (mg/dL) | 185.4±35.7 | 184.4±35.2 | 188.4±37.4 | 0.390 | 0.533 |
| TG (mg/dL) | 117.0 (83.5, 159.5) | 118.0 (84.0, 157.0) | 105.5 (73.5, 159.8) | 1.052 | 0.305 |
| HDL-C (mg/dL) | 50.2±13.2 | 49.9±13.0 | 51.1±13.8 | 0.314 | 0.576 |
| LDL-C (mg/dL) | 110.1±28.5 | 109.3±28.3 | 112.1±29.4 | 0.394 | 0.531 |
| HbA1C (%) | 6.0 (5.7, 6.7) | 6.0 (5.6, 6.6) | 6.0 (5.7, 7.0) | 2.139 | 0.144 |
| CRP (mg/dL) | 0.1 (0.0, 0.3) | 0.1 (0.0, 0.3) | 0.1 (0.1, 0.3) | 1.240 | 0.266 |
| LVEF (%) | 63.2±9.8 | 65.0±7.3 | 58.6±13.6 | 18.205 | <0.001 |
| Cerebral infarction [n (%)] | 35 (17.2) | 27 (18.1) | 8 (14.5) | 0.361 | 0.548 |
| Peripheral arterial disease [n (%)] | 53 (26.0) | 42 (28.2) | 11 (20) | 1.400 | 0.237 |
| Atrial fibrillation [n (%)] | 26 (12.7) | 13 (8.7) | 13 (23.6) | 8.032 | 0.005 |
| Hypertension [n (%)] | 151 (74.0) | 111 (74.5) | 40 (72.7) | 0.065 | 0.798 |
| Dyslipidemia [n (%)] | 104 (51.0) | 78 (52.3) | 26 (47.3) | 0.414 | 0.520 |
| Diabetes [n (%)] | 73 (35.8) | 50 (33.6) | 23 (41.8) | 1.193 | 0.275 |
| Variable | Total (n=204) | Control group (n=149) | β-blocker group (n=55) | Statistic | P |
|---|---|---|---|---|---|
| Coronary angiography status | |||||
| LMT lesions | 13 (6.4) | 10 (6.7) | 3 (5.5) | 1.000 | |
| Bifurcation lesions | 102 (50.0) | 70 (47) | 32 (58.2) | 2.016 | 0.156 |
| Ostial lesions | 30 (14.7) | 22 (14.8) | 8 (14.5) | 0.002 | 0.969 |
| Calcified lesions | 29 (14.2) | 21 (14.1) | 8 (14.5) | 0.007 | 0.935 |
| CTO lesions | 12 (5.9) | 9 (6) | 3 (5.5) | - | 1.000 |
| Multi-vessel lesions | 53 (26.0) | 38 (25.5) | 15 (27.3) | 0.065 | 0.798 |
| Stent | - | 0.171 | |||
| BMS | 11 (5.4) | 6 (4) | 5 (9.1) | ||
| DES | 193 (94.6) | 143 (96) | 50 (90.9) | ||
| Medication | |||||
| Aspirin | 202 (99.0) | 148 (99.3) | 54 (98.2) | - | 0.467 |
| Thienopiridines | 200 (98.0) | 147 (98.7) | 53 (96.4) | - | 0.294 |
| Warfarin | 5 (2.5) | 2 (1.3) | 3 (5.5) | - | 0.123 |
| NOAC | 21 (10.3) | 12 (8.1) | 9 (16.4) | 3.004 | 0.083 |
| Ezetimibe | 3 (1.5) | 3 (2) | 0 (0) | - | 0.565 |
| PPI | 134 (65.7) | 104 (69.8) | 30 (54.5) | 4.147 | 0.042 |
| Statin | 111 (54.4) | 86 (57.7) | 25 (45.5) | 2.436 | 0.119 |
| ACEI | 19 (9.3) | 14 (9.4) | 5 (9.1) | 0.004 | 0.947 |
| ARB | 88 (43.1) | 66 (44.3) | 22 (40) | 0.302 | 0.583 |
| MRA | 11 (5.4) | 5 (3.4) | 6 (10.9) | - | 0.072 |
| Outcomes | |||||
| All-cause death | 18 (8.8) | 13 (8.7) | 5 (9.1) | - | 1.000 |
| MACEs | 19 (9.3) | 15 (10.1) | 4 (7.3) | 0.371 | 0.542 |
| Cardiovascular death | 6 (2.9) | 4 (2.7) | 2 (3.6) | - | 0.662 |
| Non-fatal MI | 3 (1.5) | 3 (2.0) | 0 (0.0) | - | 0.565 |
| Non-fatal stroke | 11 (5.4) | 9 (6.0) | 2 (3.6) | - | 0.731 |
Tab.2 Comparation of angiographic characteristics, medication and clinical outcomes [n (%)]
| Variable | Total (n=204) | Control group (n=149) | β-blocker group (n=55) | Statistic | P |
|---|---|---|---|---|---|
| Coronary angiography status | |||||
| LMT lesions | 13 (6.4) | 10 (6.7) | 3 (5.5) | 1.000 | |
| Bifurcation lesions | 102 (50.0) | 70 (47) | 32 (58.2) | 2.016 | 0.156 |
| Ostial lesions | 30 (14.7) | 22 (14.8) | 8 (14.5) | 0.002 | 0.969 |
| Calcified lesions | 29 (14.2) | 21 (14.1) | 8 (14.5) | 0.007 | 0.935 |
| CTO lesions | 12 (5.9) | 9 (6) | 3 (5.5) | - | 1.000 |
| Multi-vessel lesions | 53 (26.0) | 38 (25.5) | 15 (27.3) | 0.065 | 0.798 |
| Stent | - | 0.171 | |||
| BMS | 11 (5.4) | 6 (4) | 5 (9.1) | ||
| DES | 193 (94.6) | 143 (96) | 50 (90.9) | ||
| Medication | |||||
| Aspirin | 202 (99.0) | 148 (99.3) | 54 (98.2) | - | 0.467 |
| Thienopiridines | 200 (98.0) | 147 (98.7) | 53 (96.4) | - | 0.294 |
| Warfarin | 5 (2.5) | 2 (1.3) | 3 (5.5) | - | 0.123 |
| NOAC | 21 (10.3) | 12 (8.1) | 9 (16.4) | 3.004 | 0.083 |
| Ezetimibe | 3 (1.5) | 3 (2) | 0 (0) | - | 0.565 |
| PPI | 134 (65.7) | 104 (69.8) | 30 (54.5) | 4.147 | 0.042 |
| Statin | 111 (54.4) | 86 (57.7) | 25 (45.5) | 2.436 | 0.119 |
| ACEI | 19 (9.3) | 14 (9.4) | 5 (9.1) | 0.004 | 0.947 |
| ARB | 88 (43.1) | 66 (44.3) | 22 (40) | 0.302 | 0.583 |
| MRA | 11 (5.4) | 5 (3.4) | 6 (10.9) | - | 0.072 |
| Outcomes | |||||
| All-cause death | 18 (8.8) | 13 (8.7) | 5 (9.1) | - | 1.000 |
| MACEs | 19 (9.3) | 15 (10.1) | 4 (7.3) | 0.371 | 0.542 |
| Cardiovascular death | 6 (2.9) | 4 (2.7) | 2 (3.6) | - | 0.662 |
| Non-fatal MI | 3 (1.5) | 3 (2.0) | 0 (0.0) | - | 0.565 |
| Non-fatal stroke | 11 (5.4) | 9 (6.0) | 2 (3.6) | - | 0.731 |
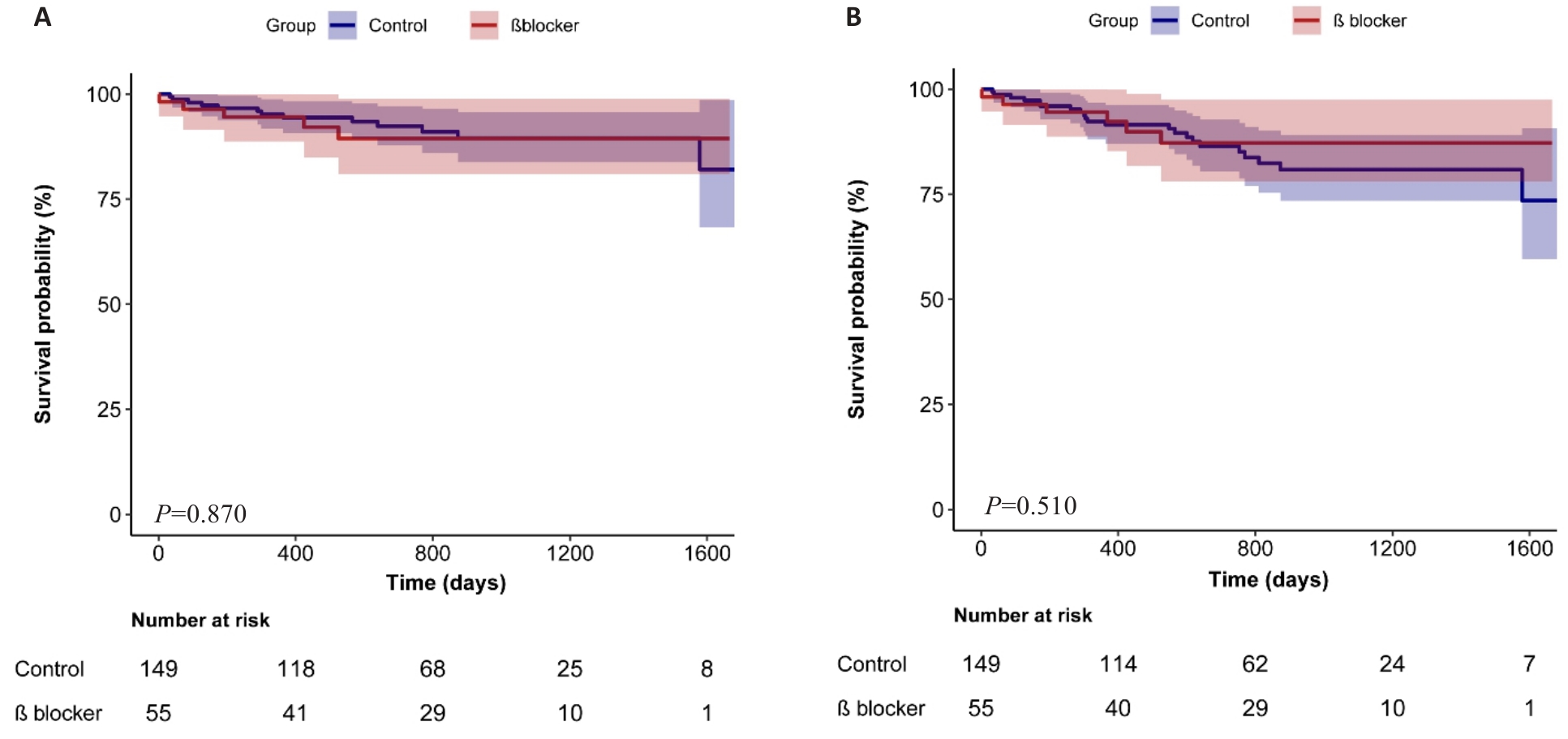
Fig.1 Kaplan-Meier survival curves of the patients with and without post-PCI β-blocker. A: All-cause mortality. B: MACEs.
| Model | All-cause death | MACEs | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Univariate Cox regression | 1.08 (0.38-3.04) | 0.881 | 0.73 (0.30-1.81) | 0.498 |
| Multivariate Cox regression* | 0.81 (0.24-2.72) | 0.735 | 0.62 (0.22-1.69) | 0.348 |
| PS adjustment | 0.69 (0.21-2.27) | 0.542 | 0.56 (0.20-1.52) | 0.255 |
| PS matching | 1.49 (0.25-8.91) | 0.664 | 0.59 (0.17-2.10) | 0.415 |
| IPTW | 0.60 (0.17-2.11) | 0.383 | 0.53 (0.20-1.45) | 0.244 |
| SMRW | 0.91 (0.33-2.54) | 0.881 | 0.64 (0.26-1.58) | 0.386 |
Tab.3 Comparison of outcomes of the patients in the two groups using Cox regression and propensity score
| Model | All-cause death | MACEs | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Univariate Cox regression | 1.08 (0.38-3.04) | 0.881 | 0.73 (0.30-1.81) | 0.498 |
| Multivariate Cox regression* | 0.81 (0.24-2.72) | 0.735 | 0.62 (0.22-1.69) | 0.348 |
| PS adjustment | 0.69 (0.21-2.27) | 0.542 | 0.56 (0.20-1.52) | 0.255 |
| PS matching | 1.49 (0.25-8.91) | 0.664 | 0.59 (0.17-2.10) | 0.415 |
| IPTW | 0.60 (0.17-2.11) | 0.383 | 0.53 (0.20-1.45) | 0.244 |
| SMRW | 0.91 (0.33-2.54) | 0.881 | 0.64 (0.26-1.58) | 0.386 |
| [1] | Chong B, Jayabaskaran J, Jauhari SM, et al. Global burden of cardiovascular diseases: projections from 2025 to 2050[J]. Eur J Prev Cardiol, 2025, 32(11): 1001-15. doi:10.1093/eurjpc/zwae281 |
| [2] | 中国心血管健康与疾病报告2024概要 [J]. 中国循环杂志, 2025, 40 (6): 521-59. |
| [3] | Navarese EP, Lansky AJ, Kereiakes DJ, et al. Cardiac mortality in patients randomised to elective coronary revascularisation plus medical therapy or medical therapy alone: a systematic review and meta-analysis[J]. Eur Heart J, 2021, 42(45): 4638-51. doi:10.1093/eurheartj/ehab246 |
| [4] | Hahn JY, Song YB, Oh JH, et al. Effect of P2Y12 inhibitor monotherapy vs dual antiplatelet therapy on cardiovascular events in patients undergoing percutaneous coronary intervention: the SMART-CHOICE randomized clinical trial[J]. JAMA, 2019, 321(24): 2428-37. doi:10.1001/jama.2019.8146 |
| [5] | Boberg J, Larsen FF, Pehrsson SK. The effects of beta blockade with (epanolol) and without (atenolol) intrinsic sympathomimetic activity in stable angina pectoris. The Visacor Study Group[J]. Clin Cardiol, 1992, 15(8): 591-5. doi:10.1002/clc.4960150808 |
| [6] | Vantrimpont P, Rouleau JL, Wun CC, et al. Additive beneficial effects of beta-blockers to angiotensin-converting enzyme inhibitors in the Survival and Ventricular Enlargement (SAVE) Study. SAVE Investigators[J]. J Am Coll Cardiol, 1997, 29(2): 229-36. doi:10.1016/s0735-1097(96)00489-5 |
| [7] | Dargie HJ. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial[J]. Lancet, 2001, 357(9266): 1385-90. doi:10.1016/s0140-6736(00)04560-8 |
| [8] | Park CS, Yang HM, Ki YJ, et al. Left ventricular ejection fraction 1 year after acute myocardial infarction identifies the benefits of the long-term use of β-blockers: analysis of data from the KAMIR-NIH registry[J]. Circ Cardiovasc Interv, 2021, 14(4): e010159. doi:10.1161/circinterventions.120.010159 |
| [9] | Packer M, Fowler MB, Roecker EB, et al. Effect of carvedilol on the morbidity of patients with severe chronic heart failure: results of the carvedilol prospective randomized cumulative survival (COPERNICUS) study[J]. Circulation, 2002, 106(17): 2194-9. doi:10.1161/01.cir.0000035653.72855.bf |
| [10] | Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the management of patients with chronic coronary disease: a report of the American heart association/American college of cardiology joint committee on clinical practice guidelines[J]. Circulation, 2023, 148(9): e9-e119. doi:10.1161/cir.0000000000001183 |
| [11] | Vrints C, Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes[J]. Eur Heart J, 2024, 45(36): 3415-537. |
| [12] | 中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 中国慢性冠脉综合征患者诊断及管理指南[J]. 中华心血管病杂志, 2024, 52(6): 589-614. |
| [13] | Park J, Han JK, Kang J, et al. The clinical impact of β-blocker therapy on patients with chronic coronary artery disease after percutaneous coronary intervention[J]. Korean Circ J, 2022, 52(7): 544-55. doi:10.4070/kcj.2021.0395 |
| [14] | Khan SU, Akbar UA, Khan MS, et al. Beta-blockers after PCI for stable coronary artery disease and preserved left ventricular ejection fraction[J]. JACC Adv, 2025, 4(2): 101566. doi:10.1016/j.jacadv.2024.101566 |
| [15] | Consortium TC, Cao YN, Li L, et al. The ChinaMAP analytics of deep whole genome sequences in 10, 588 individuals[J]. Cell Res, 2020, 30(9): 717-31. doi:10.1038/s41422-020-0322-9 |
| [16] | Hwang MJ. Demographic change in east Asia: cultural legacies, contemporary challenges, and strategic responses[J]. China Popul Dev Stud, 2025, 9(2): 142-50. doi:10.1007/s42379-025-00198-3 |
| [17] | Suzuki S, Hashizume N, Kanzaki Y, et al. Prognostic significance of serum albumin in patients with stable coronary artery disease treated by percutaneous coronary intervention[J]. PLoS One, 2019, 14(7): e0219044. doi:10.1371/journal.pone.0219044 |
| [18] | Kim J, Kang D, Park H, et al. Long-term β‑blocker therapy and clinical outcomes after acute myocardial infarction in patients without heart failure: nationwide cohort study[J]. Eur Heart J, 2020, 41(37): 3521-9. doi:10.1093/eurheartj/ehaa376 |
| [19] | Dahl Aarvik M, Sandven I, Dondo TB, et al. Effect of oral β-blocker treatment on mortality in contemporary post-myocardial infarction patients: a systematic review and meta-analysis[J]. Eur Heart J Cardiovasc Pharmacother, 2019, 5(1): 12-20. doi:10.1093/ehjcvp/pvy034 |
| [20] | Ishak D, Aktaa S, Lindhagen L, et al. Association of beta-blockers beyond 1 year after myocardial infarction and cardiovascular outcomes[J]. Heart, 2023, 109(15): 1159-65. doi:10.1136/heartjnl-2022-322115 |
| [21] | Neumann A, Maura G, Weill A, et al. Clinical events after discontinuation of β‑blockers in patients without heart failure optimally treated after acute myocardial infarction: a cohort study on the French healthcare databases[J]. Circ Cardiovasc Qual Outcomes, 2018, 11(4): e004356. doi:10.1161/circoutcomes.117.004356 |
| [22] | Ibáñez B, Latini R, Rosselló X, et al. Beta-blockers after myocardial infarction without reduced ejection fraction[J]. N Engl J Med, 2025. |
| [23] | Munkhaugen J, Kristensen AMD, Halvorsen S, et al. Beta-blockers after myocardial infarction in patients without heart failure[J]. N Engl J Med, 2025. . |
| [24] | Sorbets E, Steg PG, Young R, et al. β-blockers, calcium antagonists, and mortality in stable coronary artery disease: an international cohort study[J]. Eur Heart J, 2019, 40(18): 1399-407. doi:10.1093/eurheartj/ehy811 |
| [25] | Bangalore S, Steg G, Deedwania P, et al. β-Blocker use and clinical outcomes in stable outpatients with and without coronary artery disease[J]. JAMA, 2012, 308(13): 1340-9. doi:10.1001/jama.2012.12559 |
| [26] | Godoy LC, Farkouh ME, Austin PC, et al. Association of beta-blocker therapy with cardiovascular outcomes in patients with stable ischemic heart disease[J]. J Am Coll Cardiol, 2023, 81(24): 2299-311. doi:10.1016/j.jacc.2023.04.021 |
| [27] | 应用β肾上腺素能受体阻滞剂规范治疗冠心病的中国专家共识[J]. 中国循环杂志, 2020, 35(02): 108-23. |
| [28] | Jin P, Ma J, Wu P, et al. PCSK9 inhibition mitigates vulnerable plaque formation induced by hyperhomocysteinemia through regulating lipid metabolism and inflammation[J]. Biochem Pharmacol, 2025, 239: 117031. doi:10.1016/j.bcp.2025.117137 |
| [29] | Biccirè FG, Häner J, Losdat S, et al. Concomitant coronary atheroma regression and stabilization in response to lipid-lowering therapy[J]. J Am Coll Cardiol, 2023, 82(18): 1737-47. doi:10.1016/j.jacc.2023.08.019 |
| [30] | Montalto C, Costa F, Leonardi S, et al. Dual antiplatelet therapy duration after percutaneous coronary intervention in patients with indication to oral anticoagulant therapy. A systematic review and meta-analysis of randomized controlled trials[J]. Eur Heart J Cardiovasc Pharmacother, 2023, 9(3): 220-30. doi:10.1093/ehjcvp/pvac065 |
| [31] | Kereiakes DJ. Dual antiplatelet therapy duration following percutaneous coronary intervention: time for a change[J]. J Soc Cardiovasc Angiogr Interv, 2025, 4(2): 102510. doi:10.1016/j.jscai.2024.102510 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||