Journal of Southern Medical University ›› 2024, Vol. 44 ›› Issue (6): 1033-1039.doi: 10.12122/j.issn.1673-4254.2024.06.03
Ke LIU1,2( ), Zhenyan MA1, Lei FU1, Liping ZHANG2, Xin A2, Shaobo XIAO1, Zhen ZHANG1, Hongbo ZHANG3, Lei ZHAO3, Geng QIAN1,2()
), Zhenyan MA1, Lei FU1, Liping ZHANG2, Xin A2, Shaobo XIAO1, Zhen ZHANG1, Hongbo ZHANG3, Lei ZHAO3, Geng QIAN1,2()
Received:2024-01-16
Online:2024-06-20
Published:2024-07-01
Contact:
Geng QIAN
E-mail:997036483@qq.com;qiangeng9396@263.net
Ke LIU, Zhenyan MA, Lei FU, Liping ZHANG, Xin A, Shaobo XIAO, Zhen ZHANG, Hongbo ZHANG, Lei ZHAO, Geng QIAN. Predictive value of global longitudinal strain measured by cardiac magnetic resonance imaging for left ventricular remodeling after acute ST-segment elevation myocardial infarction: a multi-centered prospective study[J]. Journal of Southern Medical University, 2024, 44(6): 1033-1039.
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.j-smu.com/EN/10.12122/j.issn.1673-4254.2024.06.03
| Index | Total population (n=403) | LVR group (n=101) | non-LVR group (n=302) | P |
|---|---|---|---|---|
| Female [n (%)] | 54 (13.4) | 11 (10.9) | 43 (14.2) | 0.393 |
| Age (year) | 56.8±10.7 | 56.7±11.5 | 56.9±10.4 | 0.919 |
| BMI (kg/m2) | 25.9±7.6 | 25.6±3.3 | 26.0±8.6 | 0.626 |
| SBP (mmHg) | 126±22 | 126±21 | 126±22 | 0.832 |
| DBP (mmHg) | 77±16 | 79±16 | 77±16 | 0.346 |
| Heart rate (beat/min) | 79±14 | 82±14 | 79±14 | 0.039 |
| Current smoker [n (%)] | 210 (52.1) | 47 (46.5) | 163 (54.0) | 0.422 |
| Hypertension [n (%)] | 201 (49.9) | 57 (56.4) | 144 (47.7) | 0.128 |
| Diabetes [n (%)] | 87 (21.6) | 23 (22.8) | 64 (21.2) | 0.738 |
| Hyperlipidemia [n (%)] | 81 (20.1) | 20 (19.8) | 61 (20.2) | 0.931 |
| Hb (g/L) | 146.5±15.7 | 146.2±15.6 | 146.6±15.8 | 0.821 |
| WBC (109/L) | 10.8±3.3 | 11.5±3.5 | 10.6±3.2 | 0.022 |
| PLT (109/L) | 229±73 | 238±69 | 227±74 | 0.184 |
| LDL (mmol/L) | 3.08±0.93 | 3.18±1.02 | 3.06±0.90 | 0.276 |
| Cr (μmol/L) | 77.30±18.58 | 78.93±17.78 | 76.76±18.84 | 0.310 |
| CK-MB peaks (ng/mL) | 166 (79.9-297.0) | 237.8 (104.5-374.7) | 150.9 (73.9-281.1) | 0.001 |
| TIMI flow before PCI [n (%)] | 0.243 | |||
| 0 | 296 (73.4) | 81 (80.2) | 215 (71.2) | |
| 1 | 27 (6.7) | 7 (6.9) | 20 (6.6) | |
| 2 | 35 (8.7) | 6 (6.0) | 29 (9.6) | |
| 3 | 45 (11.2) | 7 (6.9) | 38 (12.6) | |
| Number of affected vessels [n (%)] | 0.694 | |||
| 1 | 186 (46.2) | 50 (49.5) | 136 (45.1) | |
| 2 | 103 (25.5) | 25 (24.8) | 78 (25.8) | |
| 3 | 114 (28.3) | 26 (25.7) | 88 (29.1) | |
| Killp rating [n(%)] | 0.052 | |||
| 1 | 341 (84.6) | 79 (78.2) | 262 (86.8) | |
| 2 | 50 (12.4) | 16 (15.8) | 34 (11.3) | |
| 3 | 12 (3.0) | 6 (5.9) | 6 (2.0) | |
| CMR parameter (%) | ||||
| GLS | -11.60 (-13.93- -9.34) | -9.24 (-11.15- -7.12) | -12.36 (-14.41- -10.16) | <0.001 |
| GCS | -13.90 (-16.01- -11.7) | -11.90 (-14.11- -9.72) | -14.40 (-16.29- -12.51) | <0.001 |
| GRS | 21.39 (17.15-25.59) | 17.39 (13.66-22.05) | 22.73 (18.63-26.01) | <0.001 |
| IS | 22.10 (13.50-32.16) | 29.21 (20.21-37.95) | 20.08 (11.93-30.37) | <0.001 |
| LVEF | 47.84 (40.24-54.13) | 39.88 (34.81-47.28) | 49.79 (43.11-55.59) | <0.001 |
Tab.1 Comparison of clinical data and CMR parameters between the two groups
| Index | Total population (n=403) | LVR group (n=101) | non-LVR group (n=302) | P |
|---|---|---|---|---|
| Female [n (%)] | 54 (13.4) | 11 (10.9) | 43 (14.2) | 0.393 |
| Age (year) | 56.8±10.7 | 56.7±11.5 | 56.9±10.4 | 0.919 |
| BMI (kg/m2) | 25.9±7.6 | 25.6±3.3 | 26.0±8.6 | 0.626 |
| SBP (mmHg) | 126±22 | 126±21 | 126±22 | 0.832 |
| DBP (mmHg) | 77±16 | 79±16 | 77±16 | 0.346 |
| Heart rate (beat/min) | 79±14 | 82±14 | 79±14 | 0.039 |
| Current smoker [n (%)] | 210 (52.1) | 47 (46.5) | 163 (54.0) | 0.422 |
| Hypertension [n (%)] | 201 (49.9) | 57 (56.4) | 144 (47.7) | 0.128 |
| Diabetes [n (%)] | 87 (21.6) | 23 (22.8) | 64 (21.2) | 0.738 |
| Hyperlipidemia [n (%)] | 81 (20.1) | 20 (19.8) | 61 (20.2) | 0.931 |
| Hb (g/L) | 146.5±15.7 | 146.2±15.6 | 146.6±15.8 | 0.821 |
| WBC (109/L) | 10.8±3.3 | 11.5±3.5 | 10.6±3.2 | 0.022 |
| PLT (109/L) | 229±73 | 238±69 | 227±74 | 0.184 |
| LDL (mmol/L) | 3.08±0.93 | 3.18±1.02 | 3.06±0.90 | 0.276 |
| Cr (μmol/L) | 77.30±18.58 | 78.93±17.78 | 76.76±18.84 | 0.310 |
| CK-MB peaks (ng/mL) | 166 (79.9-297.0) | 237.8 (104.5-374.7) | 150.9 (73.9-281.1) | 0.001 |
| TIMI flow before PCI [n (%)] | 0.243 | |||
| 0 | 296 (73.4) | 81 (80.2) | 215 (71.2) | |
| 1 | 27 (6.7) | 7 (6.9) | 20 (6.6) | |
| 2 | 35 (8.7) | 6 (6.0) | 29 (9.6) | |
| 3 | 45 (11.2) | 7 (6.9) | 38 (12.6) | |
| Number of affected vessels [n (%)] | 0.694 | |||
| 1 | 186 (46.2) | 50 (49.5) | 136 (45.1) | |
| 2 | 103 (25.5) | 25 (24.8) | 78 (25.8) | |
| 3 | 114 (28.3) | 26 (25.7) | 88 (29.1) | |
| Killp rating [n(%)] | 0.052 | |||
| 1 | 341 (84.6) | 79 (78.2) | 262 (86.8) | |
| 2 | 50 (12.4) | 16 (15.8) | 34 (11.3) | |
| 3 | 12 (3.0) | 6 (5.9) | 6 (2.0) | |
| CMR parameter (%) | ||||
| GLS | -11.60 (-13.93- -9.34) | -9.24 (-11.15- -7.12) | -12.36 (-14.41- -10.16) | <0.001 |
| GCS | -13.90 (-16.01- -11.7) | -11.90 (-14.11- -9.72) | -14.40 (-16.29- -12.51) | <0.001 |
| GRS | 21.39 (17.15-25.59) | 17.39 (13.66-22.05) | 22.73 (18.63-26.01) | <0.001 |
| IS | 22.10 (13.50-32.16) | 29.21 (20.21-37.95) | 20.08 (11.93-30.37) | <0.001 |
| LVEF | 47.84 (40.24-54.13) | 39.88 (34.81-47.28) | 49.79 (43.11-55.59) | <0.001 |
| Parameter | AUC | 95%CI | P | Cutoff value |
|---|---|---|---|---|
| GLS | 0.768 | 0.714-0.823 | <0.001 | -10.6% |
| GCS | 0.699 | 0.634-0.760 | <0.001 | -13.1% |
| GRS | 0.704 | 0.640-0.763 | <0.001 | 20.1% |
| IS | 0.669 | 0.606-0.729 | <0.001 | 26.8% |
| LVEF | 0.730 | 0.668-0.786 | <0.001 | 46.0% |
Tab.2 ROC curve and cutoff value of CMR parameters
| Parameter | AUC | 95%CI | P | Cutoff value |
|---|---|---|---|---|
| GLS | 0.768 | 0.714-0.823 | <0.001 | -10.6% |
| GCS | 0.699 | 0.634-0.760 | <0.001 | -13.1% |
| GRS | 0.704 | 0.640-0.763 | <0.001 | 20.1% |
| IS | 0.669 | 0.606-0.729 | <0.001 | 26.8% |
| LVEF | 0.730 | 0.668-0.786 | <0.001 | 46.0% |
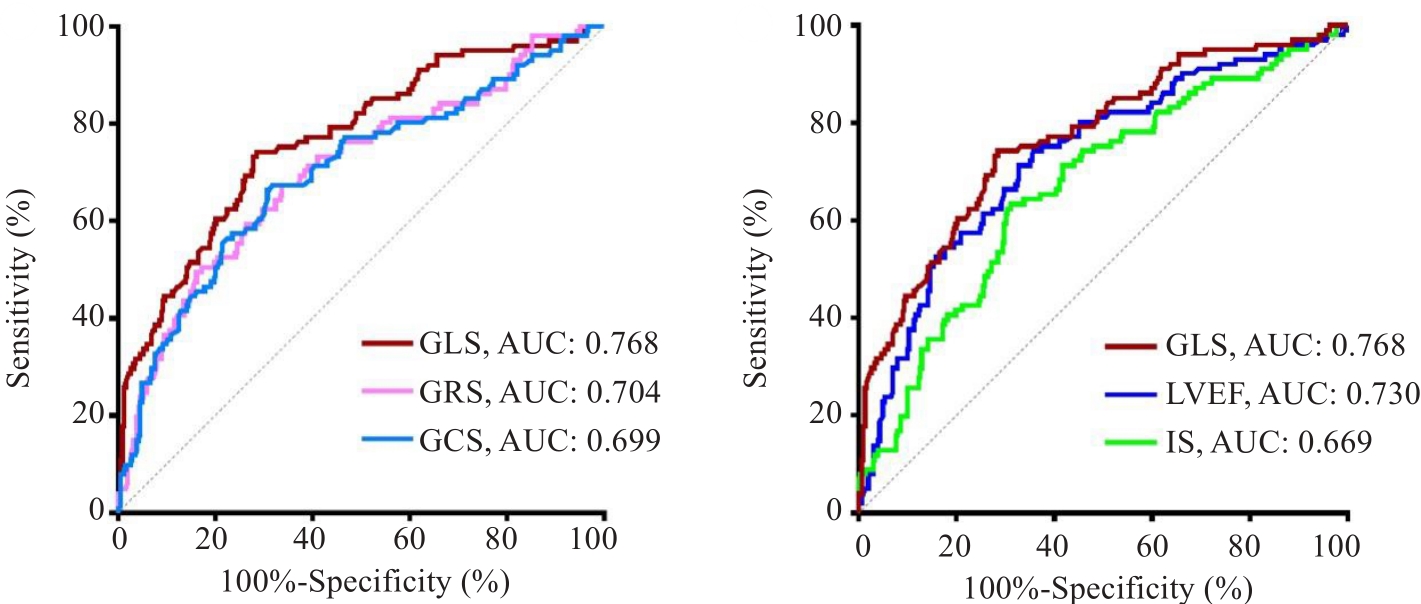
Fig.1 ROC curves of parameters.
| Parameter | Z test | AUC difference | 95%CI | P |
|---|---|---|---|---|
| GLS vs LVEF | 1.455 | 0.039 | 0.013-0.091 | 0.146 |
| GLS vs GCS | 3.063 | 0.07 | 0.025-0.114 | 0.002 |
| GLS vs GRS | 2.972 | 0.064 | 0.022-0.107 | 0.003 |
| GLS vs IS | 3.091 | 0.099 | 0.036-0.162 | 0.002 |
| LVEF vs GCS | 1.292 | 0.031 | 0.016-0.078 | 0.196 |
| LVEF vs GRS | 1.077 | 0.026 | 0.021-0.072 | 0.281 |
| LVEF vs IS | 1.833 | 0.06 | 0.004-0.124 | 0.067 |
Tab.3 Comparison of ROC curve of CMR parameters
| Parameter | Z test | AUC difference | 95%CI | P |
|---|---|---|---|---|
| GLS vs LVEF | 1.455 | 0.039 | 0.013-0.091 | 0.146 |
| GLS vs GCS | 3.063 | 0.07 | 0.025-0.114 | 0.002 |
| GLS vs GRS | 2.972 | 0.064 | 0.022-0.107 | 0.003 |
| GLS vs IS | 3.091 | 0.099 | 0.036-0.162 | 0.002 |
| LVEF vs GCS | 1.292 | 0.031 | 0.016-0.078 | 0.196 |
| LVEF vs GRS | 1.077 | 0.026 | 0.021-0.072 | 0.281 |
| LVEF vs IS | 1.833 | 0.06 | 0.004-0.124 | 0.067 |
| Parameter | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| OR 95% CI P | OR | 95% CI | P | |||
| GLS | 1.451 | 1.316-1.599 | <0.001 | 1.387 | 1.223-1.573 | <0.001 |
| GCS | 1.269 | 1.171-1.376 | <0.001 | |||
| GRS | 0.881 | 0.844-0.919 | <0.001 | |||
| IS | 1.050 | 1.031-1.069 | <0.001 | 1.022 | 1.000-1.044 | 0.053 |
| LVEF | 0.916 | 0.892-0.941 | <0.001 | 0.951 | 0.914-0.990 | 0.015 |
Tab.4 Univariate and multivariate Logistic regression analysis of CMR parameters for predicting left ventricular remodeling
| Parameter | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| OR 95% CI P | OR | 95% CI | P | |||
| GLS | 1.451 | 1.316-1.599 | <0.001 | 1.387 | 1.223-1.573 | <0.001 |
| GCS | 1.269 | 1.171-1.376 | <0.001 | |||
| GRS | 0.881 | 0.844-0.919 | <0.001 | |||
| IS | 1.050 | 1.031-1.069 | <0.001 | 1.022 | 1.000-1.044 | 0.053 |
| LVEF | 0.916 | 0.892-0.941 | <0.001 | 0.951 | 0.914-0.990 | 0.015 |
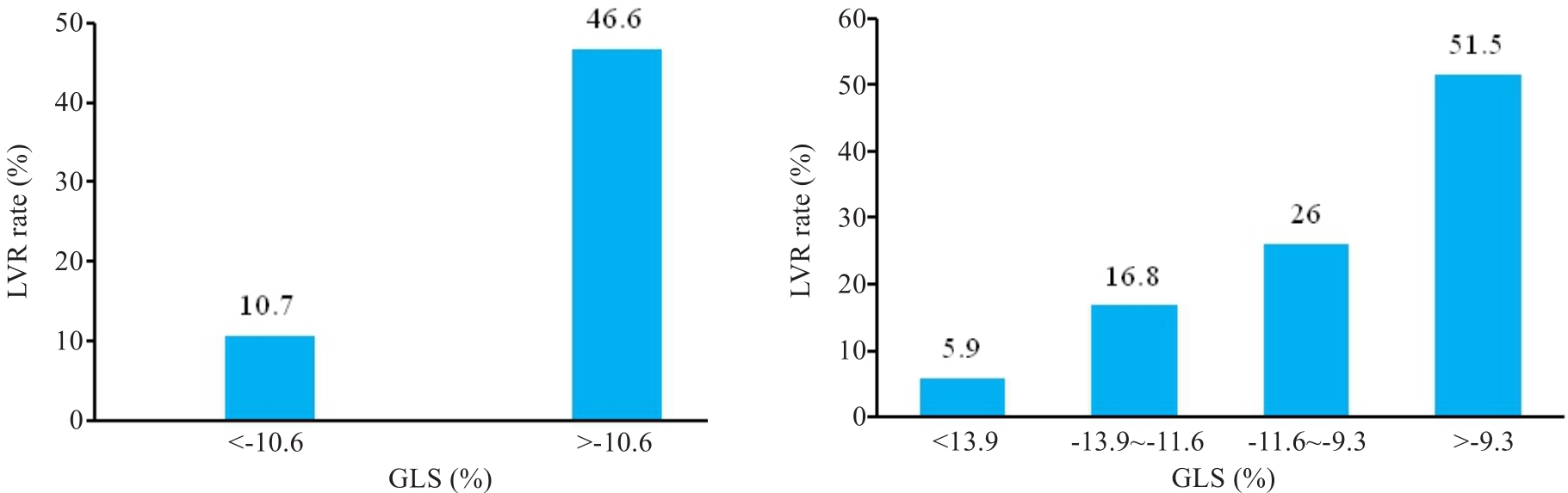
Fig.2 Incidence of LVR in GLS subgroups.
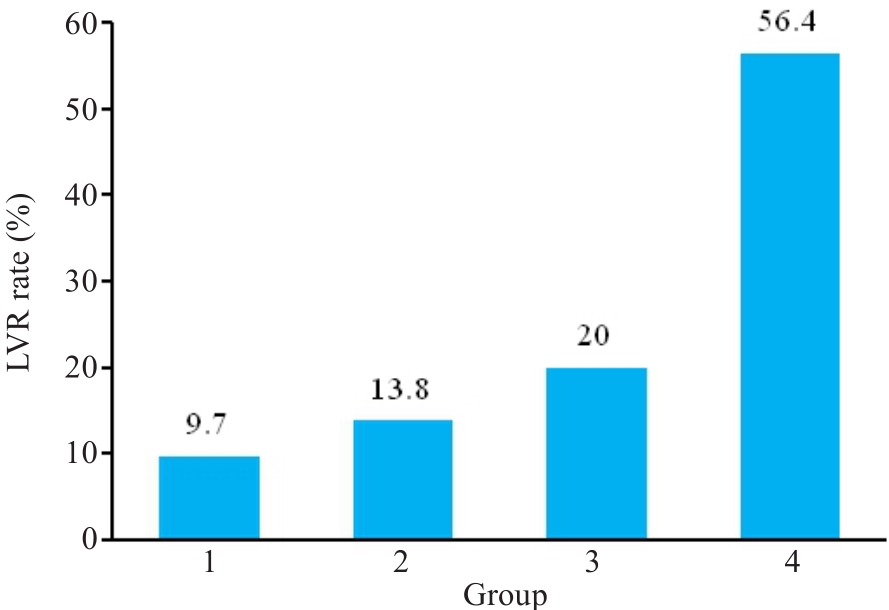
Fig.3 Incidence of LVR in patients subgrouped based on both GLS and LVEF.
| 1 | GBD Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1736-88. |
| 2 | GBD Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1204-22. |
| 3 | 中国心血管健康与疾病报告编写组. 中国心血管健康与疾病报告2022概要[J]. 中国循环杂志, 2023, 38(6): 583-612. DOI: 10.3969/j.issn.1000-3614.2023.06.001 |
| 4 | Frantz S, Hundertmark MJ, Schulz-Menger J, et al. Left ventricular remodelling post-myocardial infarction: pathophysiology, imaging, and novel therapies[J]. Eur Heart J, 2022, 43(27): 2549-61. |
| 5 | Cohn JN, Ferrari R, Sharpe N. Cardiac remodeling-concepts and clinical implications: a consensus paper from an international forum on cardiac remodeling. Behalf of an International Forum on Cardiac Remodeling [J]. J Am Coll Cardiol, 2000, 35(3): 569-582. |
| 6 | Kalam K, Otahal P, Marwick TH. Prognostic implications of global LV dysfunction: a systematic review and meta-analysis of global longitudinal strain and ejection fraction[J]. Heart, 2014, 100(21): 1673-80. |
| 7 | Biering-Sørensen T, Hoffmann S, Mogelvang R, et al. Myocardial strain analysis by 2-dimensional speckle tracking echocardiography improves diagnostics of coronary artery stenosis in stable angina pectoris[J]. Circ Cardiovasc Imaging, 2014, 7(1): 58-65. |
| 8 | Voigt JU, Cvijic M. 2- and 3-dimensional myocardial strain in cardiac health and disease[J]. JACC Cardiovasc Imaging, 2019, 12 (9): 1849-63. |
| 9 | Friedrich MG. The future of cardiovascular magnetic resonance imaging[J]. Eur Heart J, 2017, 38(22): 1698-1701. |
| 10 | Rajiah PS, François CJ, Leiner T. Cardiac MRI: state of the art[J]. Radiology, 2023, 307(3): e223008. |
| 11 | Reindl M, Tiller C, Holzknecht M, et al. Prognostic implications of global longitudinal strain by feature-tracking cardiac magnetic resonance in ST-elevation myocardial infarction[J]. Circ Cardiovasc Imaging, 2019, 12(11): e009404. |
| 12 | Morais P, Marchi A, Bogaert JA, et al. Cardiovascular magnetic resonance myocardial feature tracking using a non-rigid, elastic image registration algorithm: assessment of variability in a real-life clinical setting[J]. J Cardiovasc Magn Reson, 2017, 19(1): 24. |
| 13 | Bulluck H, Dharmakumar R, Arai AE, et al. Cardiovascular magnetic resonance in acute ST-segment-elevation myocardial infarction: recent advances, controversies, and future directions[J]. Circulation, 2018, 137(18): 1949-64. |
| 14 | Rodriguez-Palomares JF, Gavara J, Ferreira-González I, et al. Prognostic value of initial Left ventricular remodeling in patients with reperfused STEMI[J]. JACC Cardiovasc Imaging, 2019, 12(12): 2445-56. |
| 15 | Khan JN, Nazir SA, Singh A, et al. Relationship of myocardial strain and markers of myocardial injury to predict segmental recovery after acute ST-segment-elevation myocardial infarction[J]. Circ Cardiovasc Imaging, 2016, 9(6): e003457. |
| 16 | 马文坤, 李歆旎, 高程洁, 等. 心肌应变参数对急性ST段抬高型心肌梗死患者左心室重构的预测价值[J]. 海军军医大学学报, 2022, 43(5): 519-25. |
| 17 | 郭 倩, 王 晓, 郭芮丰, 等. CMR高危特征对LVEF轻度降低或保留的STEMI患者心室重构的预测价值[J]. 中华心血管病杂志, 2022, 50(9): 864-72. DOI: 10.3760/cma.j.cn112148-20220611-00462 |
| 18 | 中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 急性ST段抬高型心肌梗死诊断和治疗指南(2019)[J]. 中华心血管病杂志, 2019, 47(10): 766-83. |
| 19 | 中国医师协会胸痛专业委员会, 中华心血管病杂志(网络版)编辑委员会, 急性心肌梗死后心室重构防治专家共识起草组. 急性心肌梗死后心室重构防治专家共识[J]. 中华心血管病杂志: 网络版, 2020, 3(1): 1-7. |
| 20 | Ersbøll M, Valeur N, Mogensen UM, et al. Prediction of all-cause mortality and heart failure admissions from global left ventricular longitudinal strain in patients with acute myocardial infarction and preserved left ventricular ejection fraction[J]. J Am Coll Cardiol, 2013, 61(23): 2365-73. |
| 21 | O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines[J]. Circulation, 2013, 127(4): 529-55. |
| 22 | Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2018, 39(2): 119-77. |
| 23 | Joyce E, Hoogslag GE, Leong DP, et al. Association between left ventricular global longitudinal strain and adverse left ventricular dilatation after ST-segment-elevation myocardial infarction[J]. Circ Cardiovasc Imaging, 2014, 7(1): 74-81. |
| 24 | Eitel I, Stiermaier T, Lange T, et al. Cardiac magnetic resonance myocardial feature tracking for optimized prediction of cardiovascular events following myocardial infarction[J]. JACC Cardiovasc Imaging, 2018, 11(10): 1433-44. |
| 25 | Claus P, Omar AMS, Pedrizzetti G, et al. Tissue tracking technology for assessing cardiac mechanics: Principles, Normal Values, and Clinical Applications [J]. JACC Cardiovasc Imaging, 2015, 8(12): 1444-1460. |
| 26 | Rost C, Rost MC, Breithardt OA, et al. Relation of functional echocardiographic parameters to infarct scar transmurality by magnetic resonance imaging [J]. J Am Soc Echocardiogr, 2014, 27 |
| 27 | 767-774.. |
| 28 | Cha MJ, Lee JH, Jung HN, et al. Cardiac magnetic resonance-tissue tracking for the early prediction of adverse left ventricular remodeling after ST-segment elevation myocardial infarction[J]. Int J Cardiovasc Imaging, 2019, 35(11): 2095-102. |
| 29 | Reindl M, Tiller C, Holzknecht M, et al. Global longitudinal strain by feature tracking for optimized prediction of adverse remodeling after ST-elevation myocardial infarction[J]. Clin Res Cardiol, 2021, 110(1): 61-71. |
| [1] | CUI Jianing, LIU Wenjia, YAN Fei, ZHAO Yanan, CHEN Weijie, LUO Chuncai, ZHANG Xinghua, LI Tao. Predictive value of cardiac magnetic resonance imaging for adverse left ventricular remodeling after acute ST-segment elevation myocardial infarction [J]. Journal of Southern Medical University, 2024, 44(3): 553-562. |
| [2] | CUI Jianing, LI Runxia, LIU Xueqian, ZHAO Yanan, ZHANG Xinghua, LIU Qingbo, LI Tao. Cardiac magnetic resonance-feature tracking technique can assess cardiac function and prognosis in patients with myocardial amyloidosis [J]. Journal of Southern Medical University, 2023, 43(4): 660-666. |
| [3] |
.
Temporal variation of serum interleukin-37 and its relation with C-reactive protein in patients with acute ST-segment elevation myocardial infarction [J]. Journal of Southern Medical University, 2015, 35(12): 1751-. |
| [4] |
.
Value of assessing left ventricular longitudinal systolic peak strain in differential diagnosis of primary cardiac amyloidosis from hypertrophic cardiomyopathy [J]. Journal of Southern Medical University, 2014, 34(05): 609-. |
| [5] | ZHANG Yu-ling1,ZHOU Shu-xian1,WANG Ming-hui2,WANG Jing-feng1 Department of Cardiology1,Department of Cardiothoracic Surgery2,Second Affiliated Hospital of Sun Yat-sen University,Guangzhou 510120,China. Effects of perindopril on left ventricular remodeling and myocardial osteopontin expression in rats with myocardial infarction [J]. Journal of Southern Medical University, 2006, 26(11): 1584-1588. |
| [6] | SHEN Qian-bo, XU Ding-li, LIN Sheng, LAI Wen-yan Department of Cardiology, Nanfang Hospital, Southern Medical University, Guangzhou 510515, China. Sleep-disordered breathing and left ventricular remodeling in patients with chronic heart failure [J]. Journal of Southern Medical University, 2006, 26(04): 486-489. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||