南方医科大学学报 ›› 2024, Vol. 44 ›› Issue (9): 1783-1795.doi: 10.12122/j.issn.1673-4254.2024.09.19
刘虎1,2( ), 苏志海3, 黄成颉3, 赵磊1,2, 陈扬帆1,2, 周宇佳1,2, 吕海3, 冯前进1,2()
), 苏志海3, 黄成颉3, 赵磊1,2, 陈扬帆1,2, 周宇佳1,2, 吕海3, 冯前进1,2()
收稿日期:2024-06-14
出版日期:2024-09-20
发布日期:2024-09-30
通讯作者:
冯前进
E-mail:liuhu_smu@outlook.com;fengqj99@smu.edu.cn
作者简介:刘 虎,在读硕士研究生,E-mail: liuhu_smu@outlook.com
基金资助:
Hu LIU1,2(), Zhihai SU3, Chengjie HUANG3, Lei ZHAO1,2, Yangfan CHEN1,2, Yujia ZHOU1,2, Hai LÜ3, Qianjin FENG1,2()
Received:2024-06-14
Online:2024-09-20
Published:2024-09-30
Contact:
Qianjin FENG
E-mail:liuhu_smu@outlook.com;fengqj99@smu.edu.cn
Supported by:摘要:
目的 为有效减少L5/S1微创椎间盘射频消融术中因医师操作熟练度差异导致的治疗效果波动,实现对消融针穿刺路径风险的精确量化评估。 方法 基于自主研发的深度神经网络DWT-UNet,将L5/S1节段的MR图像精准分割为7个关键结构:L5椎骨,S1椎骨,髂骨,L5/S1节段的椎间盘、神经根、硬脊膜和皮肤。基于上述分割结果,3D建模穿刺路径的规划环境。针对穿刺的临床准则提出了6个硬性约束和6个软性约束,将医师经验通过层次分析算法量化为权重添加到穿刺路径风险函数中以提升对个例的适应性。通过提出的皮肤进针点采样子算法、Kambin三角投影面积子算法,结合层次分析算法,并运用光线追踪、CPU多线程处理和GPU并行计算等多种技术,计算出一条既符合临床硬性约束条件,又能使软性约束条件综合达到最优的穿刺路径。 结果 医师团队对算法规划的21例消融针穿刺路径进行主观评估,结果显示所有路径均满足临床基本要求(及格率100%),且95.24%的路径被评为优秀或良好。在与医师规划结果的对比中,算法在DIlium、DS1和Depth等3个指标上有不同程度的下降(P<0.05),在DDura、DL5、DN5和AKambin等4个指标上有较大提升(P<0.05)。算法规划21例的平均时间为7.97±3.73 s,而医师传统规划普遍需耗时10 min以上。 结论 本研究提出的多约束最优穿刺路径规划算法为L5/S1节段的微创椎间盘射频消融术提供了一种一站式的解决方案。经过严谨的临床评价和实验验证,该算法显示出独特的优势和广阔的临床应用潜力。
刘虎, 苏志海, 黄成颉, 赵磊, 陈扬帆, 周宇佳, 吕海, 冯前进. 面向L5/S1微创椎间盘射频消融术的多约束最优穿刺路径规划算法[J]. 南方医科大学学报, 2024, 44(9): 1783-1795.
Hu LIU, Zhihai SU, Chengjie HUANG, Lei ZHAO, Yangfan CHEN, Yujia ZHOU, Hai LÜ, Qianjin FENG. A multi-constraint optimal puncture path planning algorithm for percutaneous interventional radiofrequency thermal fusion of the L5/S1 segments[J]. Journal of Southern Medical University, 2024, 44(9): 1783-1795.
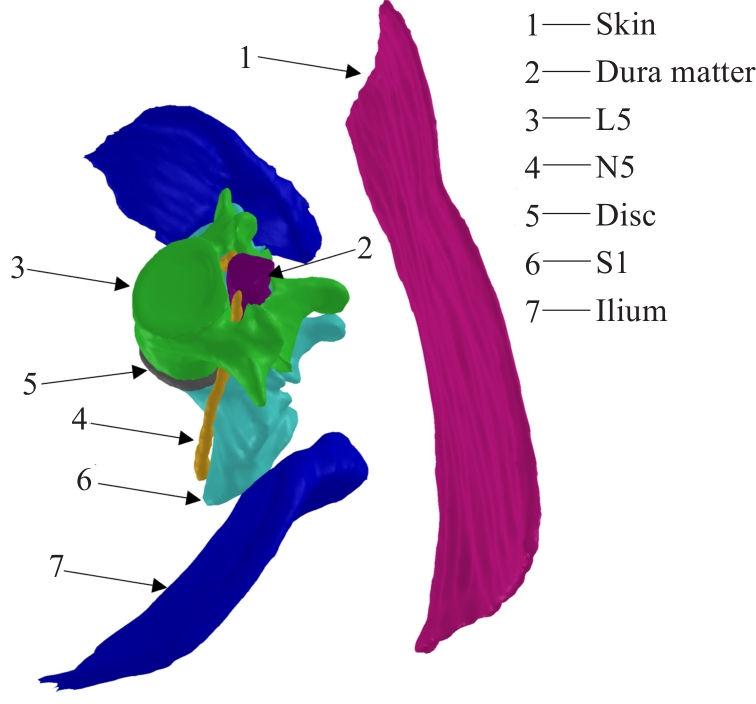
图1 3D路径规划环境模型
Fig.1 3D path planning environment.

图2 算法的整体流程
Fig.2 Overall workflow of the algorithm.
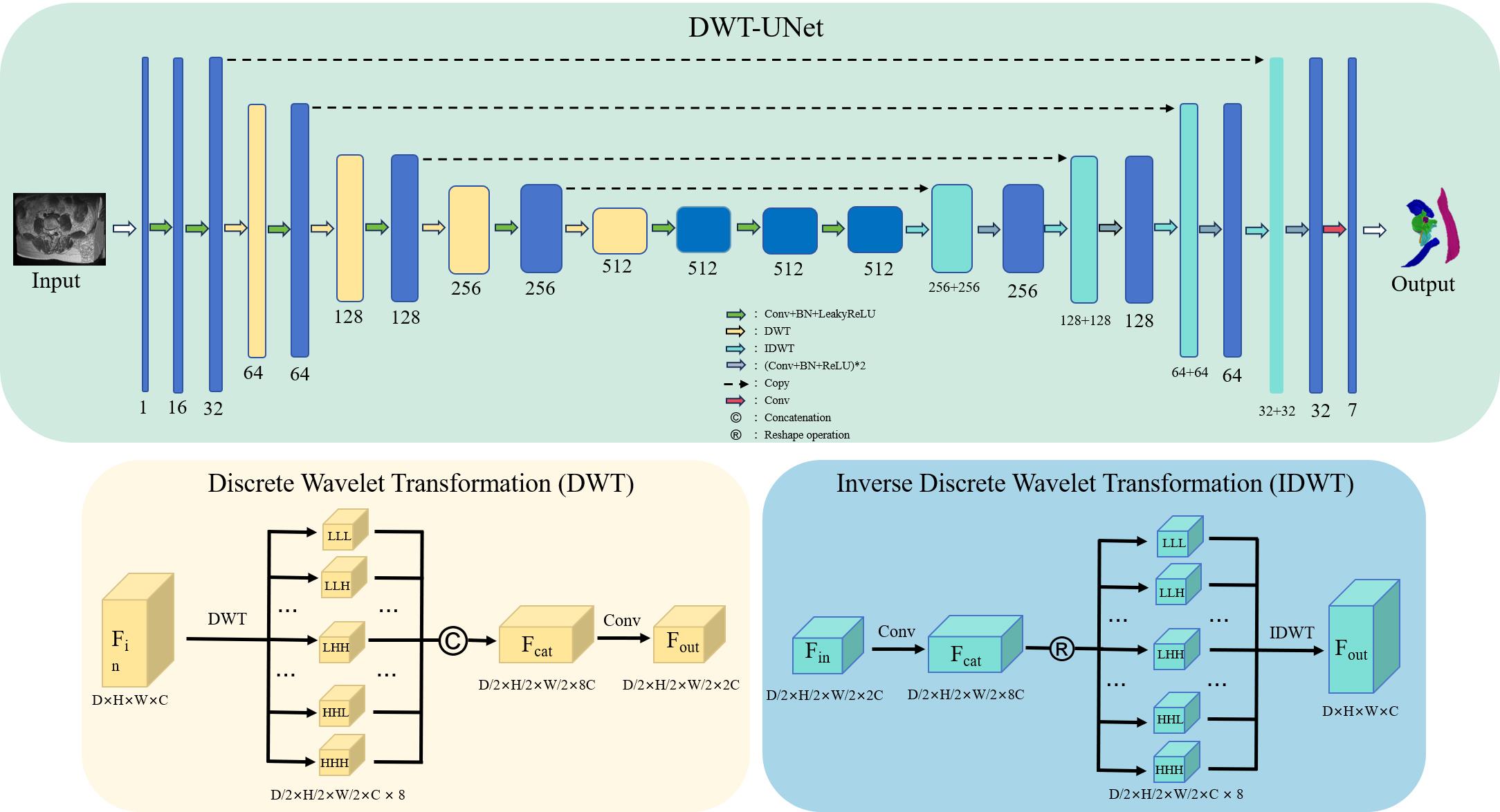
图3 DWT-UNet模型结构图
Fig.3 Structural diagram of DWT-UNet model.
| ID | Hard constraints | Soft constraints |
|---|---|---|
| A | To avoid collision with the risk-prone anatomical structures in the L5/S1 segment (including L5, S1, N5, dura mater, and ilium), ensuring a minimum clearance of 0.5mm (considering the outer diameter of a 20G needle is approximately 0.9mm) is crucial to maintain a safety margin during the procedure.[ | The distance between the puncture path and critical anatomical structures should be maximized as much as possible.[ |
| B | The puncture depth should be less than 150mm (considering the length of the puncture needle is 150mm) to ensure the ablation target can be effectively reached.[ | The puncture depth should be minimized as much as possible.[ |
| C | To prevent the phenomenon of needle slippage, the angle between the puncture path and the surface of the intervertebral disc should be greater than 20 degrees.[ | The angle between the puncture path and the surface of the intervertebral disc should be maximized as much as possible.[ |
| D* | The puncture path must traverse the intervertebral foramen. | Utilize a distance field based on bone structures to navigate and avoid densely packed bone regions. |
| E* | The puncture should be performed from the posterior (back) side. | Utilize a distance field based on neural tissue to navigate and avoid densely populated neural regions. |
| F* | The entry point of the puncture path must be located on the skin overlying the L5/S1 segment, in order to restrict the insertion range of the ablation needle. | The projected area of the Kambin's triangle should be maximized as much as possible. |
表1 PIRFT穿刺路径规划的约束
Tab.1 Constraints for path planning in radiofrequency ablation for lumbar disc herniation
| ID | Hard constraints | Soft constraints |
|---|---|---|
| A | To avoid collision with the risk-prone anatomical structures in the L5/S1 segment (including L5, S1, N5, dura mater, and ilium), ensuring a minimum clearance of 0.5mm (considering the outer diameter of a 20G needle is approximately 0.9mm) is crucial to maintain a safety margin during the procedure.[ | The distance between the puncture path and critical anatomical structures should be maximized as much as possible.[ |
| B | The puncture depth should be less than 150mm (considering the length of the puncture needle is 150mm) to ensure the ablation target can be effectively reached.[ | The puncture depth should be minimized as much as possible.[ |
| C | To prevent the phenomenon of needle slippage, the angle between the puncture path and the surface of the intervertebral disc should be greater than 20 degrees.[ | The angle between the puncture path and the surface of the intervertebral disc should be maximized as much as possible.[ |
| D* | The puncture path must traverse the intervertebral foramen. | Utilize a distance field based on bone structures to navigate and avoid densely packed bone regions. |
| E* | The puncture should be performed from the posterior (back) side. | Utilize a distance field based on neural tissue to navigate and avoid densely populated neural regions. |
| F* | The entry point of the puncture path must be located on the skin overlying the L5/S1 segment, in order to restrict the insertion range of the ablation needle. | The projected area of the Kambin's triangle should be maximized as much as possible. |
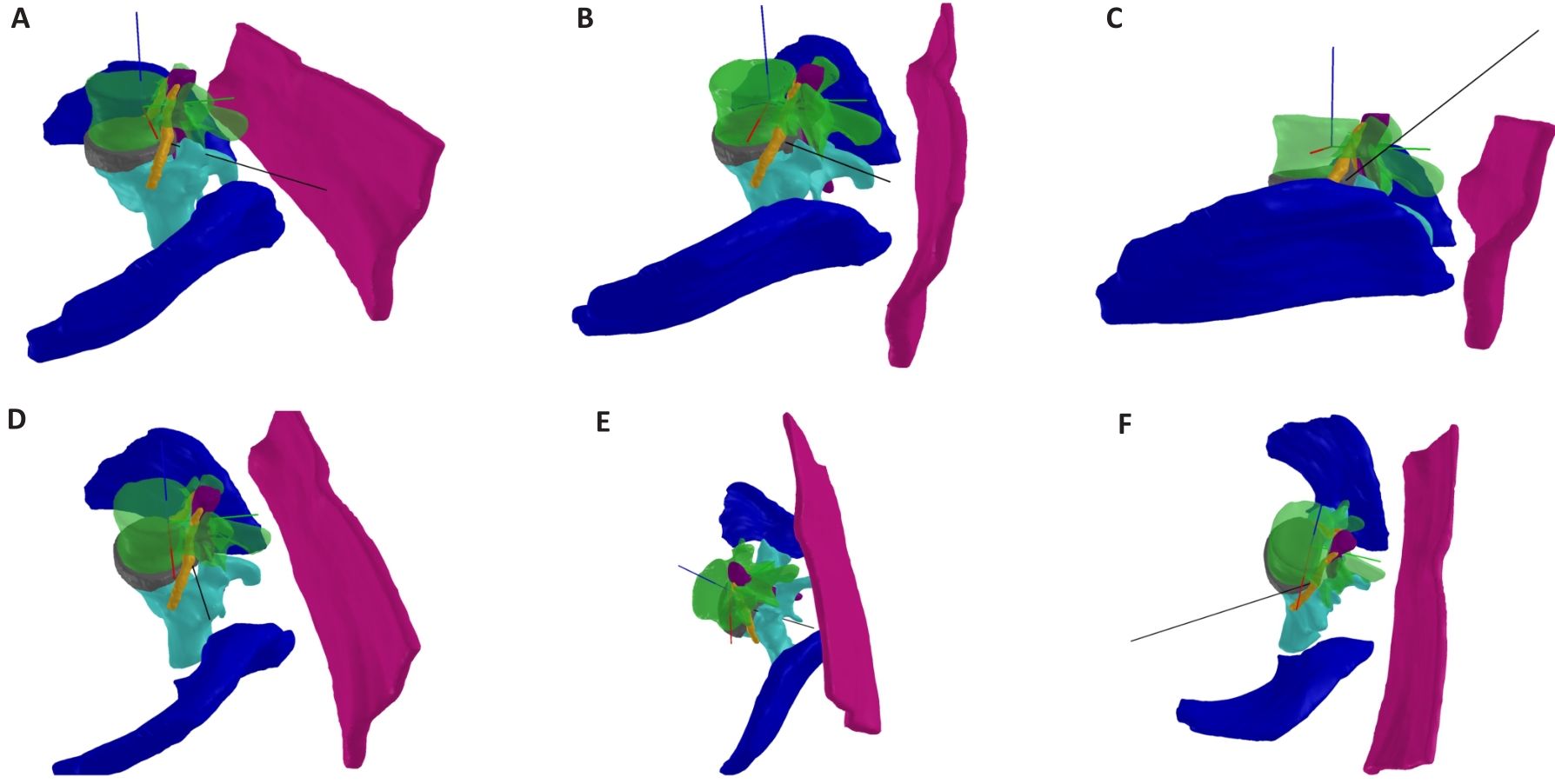
图4 违反消融针穿刺硬性约束示例图
Fig.4 Illustration of violations of hard constraints for radiofrequency ablation needle puncture. A: Collision between puncture path and S1. B: Depth greater than the maximum length. C: Entry point out of range. D: Excessively small angle. E: Path misses intervertebral foramen. F: Puncture from anterior approach.

图5 路径到关键结构示意图
Fig.5 Diagram of the path to the key structures.

图6 Kambin三角的三轴极限视角图
Fig.6 Diagram of the XYZ Axis limited perspective of the Kambin's triangle.
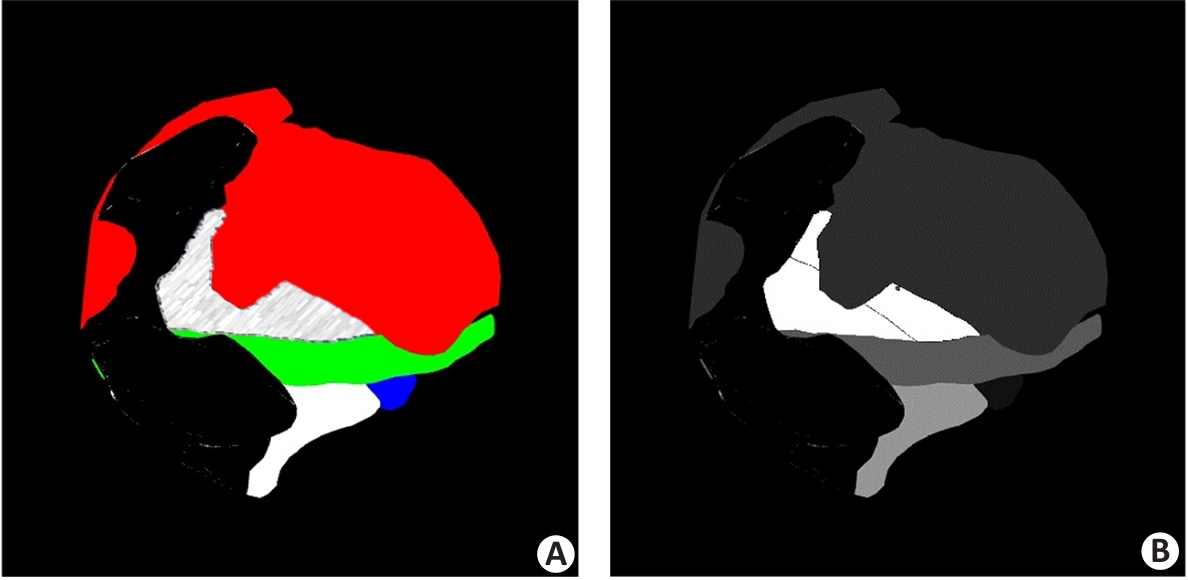
图7 Kambin三角投影示例
Fig.7 Kambin's triangle projection. A: Kambin's triangle projection area. B: Extracted Kambin's triangle region after grayscale conversion.

图8 不可行穿刺区域示例图
Fig.8 Diagram of non-feasible puncture area.
| Decision criteria | WIlium | WDura | WL5 | WN5 | WS1 | WDepth | WKambin |
|---|---|---|---|---|---|---|---|
| WIlium | 1 | 1/3 | 1/3 | 1/3 | 1/3 | 3 | 1/7 |
| WDura | 3 | 1 | 1/3 | 3 | 3 | 5 | 1/3 |
| WL5 | 3 | 3 | 1 | 5 | 5 | 7 | 1/3 |
| WN5 | 3 | 1/3 | 1/5 | 1 | 3 | 5 | 1/5 |
| WS1 | 3 | 1/3 | 1/5 | 1/3 | 1 | 5 | 1/7 |
| WDepth | 1/3 | 1/5 | 1/7 | 1/5 | 1/5 | 1 | 1/9 |
| WKambin | 7 | 3 | 3 | 5 | 7 | 9 | 1 |
表2 准则层的判断矩阵
Tab.2 Judgment matrix for criterion layer
| Decision criteria | WIlium | WDura | WL5 | WN5 | WS1 | WDepth | WKambin |
|---|---|---|---|---|---|---|---|
| WIlium | 1 | 1/3 | 1/3 | 1/3 | 1/3 | 3 | 1/7 |
| WDura | 3 | 1 | 1/3 | 3 | 3 | 5 | 1/3 |
| WL5 | 3 | 3 | 1 | 5 | 5 | 7 | 1/3 |
| WN5 | 3 | 1/3 | 1/5 | 1 | 3 | 5 | 1/5 |
| WS1 | 3 | 1/3 | 1/5 | 1/3 | 1 | 5 | 1/7 |
| WDepth | 1/3 | 1/5 | 1/7 | 1/5 | 1/5 | 1 | 1/9 |
| WKambin | 7 | 3 | 3 | 5 | 7 | 9 | 1 |
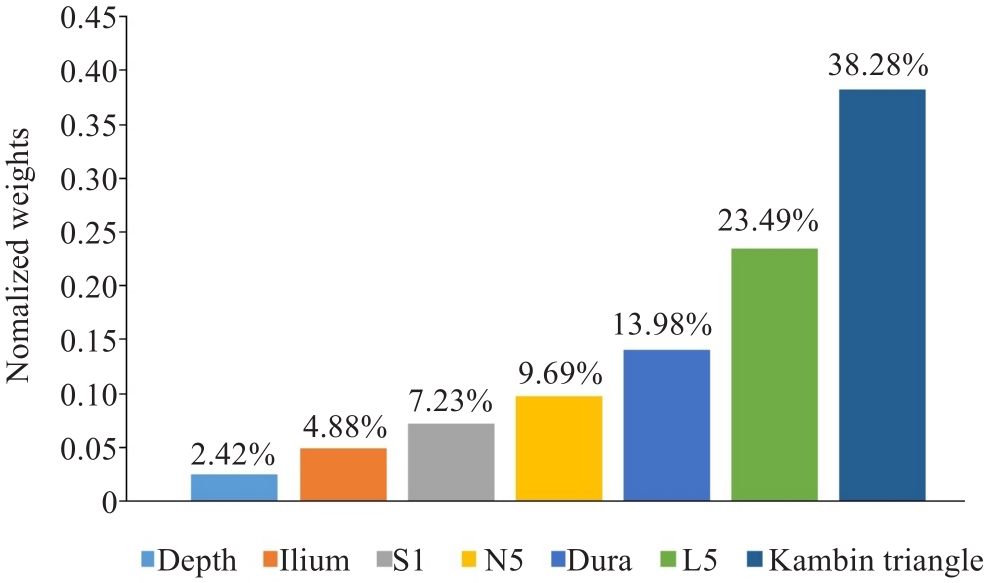
图9 权重分布复合饼柱图
Fig.9 Chart of the weight distribution.
Algorithm 1 skin insertion point sampling algorithm |
|---|
Input:Local 3D model of skin S Output:Uniform sampling needle insertion point on the skin 1:for triangle ABC in S 2: // calculate the two edge vectors of triangle ABC 3: 4: 5: // calculate the area of triangle ABC 6: 7: s 8: for j = 1, 2, 3, …, N do 9: // generate random numbers 10: if 11: 12: 13: end if 14: // sample points in triangle ABC 15: 16: add 17: end for 18: end for 19: return sampling point list |
表3 皮肤进针点采样算法
Tab.3 Algorithm for skin entry point sampling
Algorithm 1 skin insertion point sampling algorithm |
|---|
Input:Local 3D model of skin S Output:Uniform sampling needle insertion point on the skin 1:for triangle ABC in S 2: // calculate the two edge vectors of triangle ABC 3: 4: 5: // calculate the area of triangle ABC 6: 7: s 8: for j = 1, 2, 3, …, N do 9: // generate random numbers 10: if 11: 12: 13: end if 14: // sample points in triangle ABC 15: 16: add 17: end for 18: end for 19: return sampling point list |
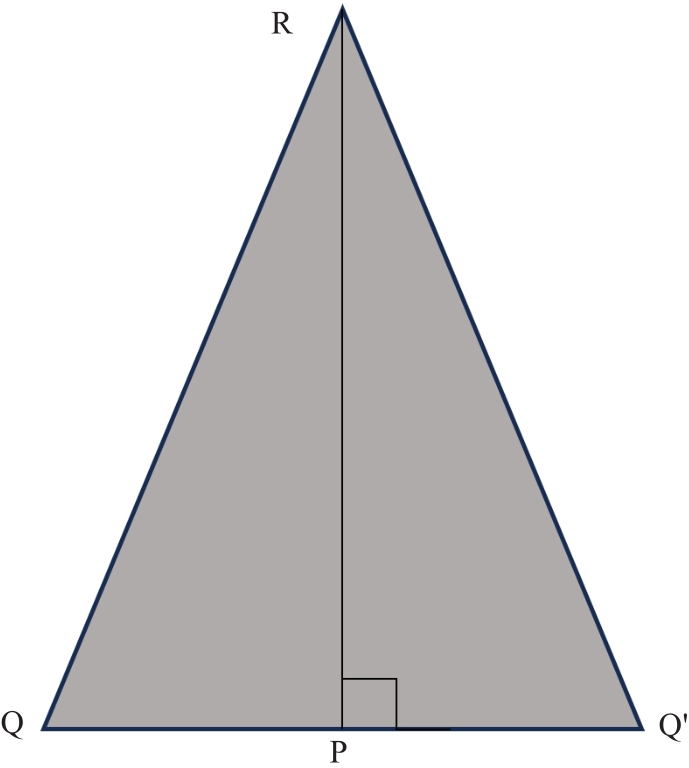
图10 误差示意图
Fig.10 Diagram of error.
| Level | Core criteria |
|---|---|
| Excellent | Satisfy all clinical hard constraints and DDura, DN5, DL5, Depth, AKambin all outperforme the manual reference path, where Depth and AKambin are allowed to have a downward deviation of no more than 2%. |
| Good | Satisfy all clinical hard constraints, with DN5 and Depth required to outperform the manual reference path, while DDura, DL5 and AKambin are allowed to have a downward deviation of no more than 5%. |
| Moderate | Satisfy all clinical hard constraints and at least 3 out of the 7 indicators (DDura, DN5, DL5, Depth, AKambin, Depth, AKambin) outperforme the manual reference path. |
| Pass | Satisfy all clinical hard constraints. |
| Fail | Violation of any clinical hard constraint condition ( |
表4 分级核心标准
Tab.4 Core criteria for grading
| Level | Core criteria |
|---|---|
| Excellent | Satisfy all clinical hard constraints and DDura, DN5, DL5, Depth, AKambin all outperforme the manual reference path, where Depth and AKambin are allowed to have a downward deviation of no more than 2%. |
| Good | Satisfy all clinical hard constraints, with DN5 and Depth required to outperform the manual reference path, while DDura, DL5 and AKambin are allowed to have a downward deviation of no more than 5%. |
| Moderate | Satisfy all clinical hard constraints and at least 3 out of the 7 indicators (DDura, DN5, DL5, Depth, AKambin, Depth, AKambin) outperforme the manual reference path. |
| Pass | Satisfy all clinical hard constraints. |
| Fail | Violation of any clinical hard constraint condition ( |
| Model | L5/S1 | ||||
|---|---|---|---|---|---|
| S1 | Disc | L5 | Dura mater | N5 | |
| nnFormer[ | 0.9434 | 0.9219 | 0.9400 | 0.9029 | 0.7933 |
| DeepLabv3[ | 0.8070 | 0.8701 | 0.8427 | 0.8161 | 0.5073 |
| U-Net++[ | 0.9462 | 0.9225 | 0.9419 | 0.9066 | 0.8012 |
| DWT-UNet (Ours) | 0.9491 | 0.9373 | 0.9488 | 0.9197 | 0.8274 |
表5 各结构的不同模型分割DSC结果
Tab.5 DSC of each structure segmented using different models
| Model | L5/S1 | ||||
|---|---|---|---|---|---|
| S1 | Disc | L5 | Dura mater | N5 | |
| nnFormer[ | 0.9434 | 0.9219 | 0.9400 | 0.9029 | 0.7933 |
| DeepLabv3[ | 0.8070 | 0.8701 | 0.8427 | 0.8161 | 0.5073 |
| U-Net++[ | 0.9462 | 0.9225 | 0.9419 | 0.9066 | 0.8012 |
| DWT-UNet (Ours) | 0.9491 | 0.9373 | 0.9488 | 0.9197 | 0.8274 |
| Model | L5/S1 | ||||
|---|---|---|---|---|---|
| S1 | Disc | L5 | Dura mater | N5 | |
| 3D U-Net[ | 0.9453 | 0.9231 | 0.9413 | 0.9035 | 0.7981 |
| 3D U-Net+DWT | 0.9491 | 0.9373 | 0.9488 | 0.9197 | 0.8274 |
| ResUNet[ | 0.9429 | 0.9221 | 0.9400 | 0.8974 | 0.7868 |
| ResUNet+DWT | 0.9466 | 0.9346 | 0.9477 | 0.9111 | 0.8160 |
| V-Net[ | 0.9404 | 0.9226 | 0.9356 | 0.8944 | 0.7814 |
| V-Net+DWT | 0.9426 | 0.9269 | 0.9431 | 0.9054 | 0.7974 |
表6 消融实验结果
Tab.6 DSC of the ablation experiment
| Model | L5/S1 | ||||
|---|---|---|---|---|---|
| S1 | Disc | L5 | Dura mater | N5 | |
| 3D U-Net[ | 0.9453 | 0.9231 | 0.9413 | 0.9035 | 0.7981 |
| 3D U-Net+DWT | 0.9491 | 0.9373 | 0.9488 | 0.9197 | 0.8274 |
| ResUNet[ | 0.9429 | 0.9221 | 0.9400 | 0.8974 | 0.7868 |
| ResUNet+DWT | 0.9466 | 0.9346 | 0.9477 | 0.9111 | 0.8160 |
| V-Net[ | 0.9404 | 0.9226 | 0.9356 | 0.8944 | 0.7814 |
| V-Net+DWT | 0.9426 | 0.9269 | 0.9431 | 0.9054 | 0.7974 |
| ID | Gender | Age (year) | Initial candidate needle insertion points | Needle insertion points that satisfy hard constraints | Depth (mm) | Clinical level |
|---|---|---|---|---|---|---|
| Case1 | Female | 53 | 43 035 | 22 097 | 123.71 | Good |
| Case2 | Female | 54 | 38 040 | 18 362 | 113.90 | Good |
| Case3 | Male | 39 | 43 925 | 11 689 | 126.46 | Good |
| Case4 | Male | 40 | 44 285 | 12 935 | 120.15 | Good |
| Case5 | Female | 26 | 38 200 | 8111 | 109.66 | Good |
| Case6 | Female | 27 | 38 995 | 10 538 | 103.67 | Excellent |
| Case7 | Female | 54 | 45 045 | 11 346 | 105.87 | Excellent |
| Case8 | Female | 32 | 38 480 | 18 646 | 87.22 | Excellent |
| Case9 | Female | 33 | 37 370 | 17 929 | 88.02 | Excellent |
| Case10 | Female | 35 | 35 070 | 15 663 | 134.82 | Good |
| Case11 | Female | 36 | 34 120 | 11 825 | 147.26 | Excellent |
| Case12 | Female | 63 | 45 875 | 12 569 | 83.74 | Moderate |
| Case13 | Female | 64 | 45 250 | 13 219 | 84.30 | Good |
| Case14 | Female | 38 | 39 495 | 9911 | 128.67 | Good |
| Case15 | Female | 39 | 38 105 | 7527 | 125.40 | Good |
| Case16 | Female | 41 | 38 240 | 6539 | 112.07 | Excellent |
| Case17 | Female | 42 | 36 895 | 3917 | 116.50 | Good |
| Case18 | Male | 33 | 43 880 | 11 475 | 130.13 | Excellent |
| Case19 | Male | 34 | 43 725 | 10 750 | 122.36 | Excellent |
| Case20 | Male | 26 | 39 115 | 10 094 | 104.42 | Excellent |
| Case21 | Male | 27 | 37 945 | 11 575 | 123.99 | Excellent |
表7 算法规划的21例穿刺路径结果
Tab.7 Parameters of the puncture paths planned by the algorithm in 21 cases
| ID | Gender | Age (year) | Initial candidate needle insertion points | Needle insertion points that satisfy hard constraints | Depth (mm) | Clinical level |
|---|---|---|---|---|---|---|
| Case1 | Female | 53 | 43 035 | 22 097 | 123.71 | Good |
| Case2 | Female | 54 | 38 040 | 18 362 | 113.90 | Good |
| Case3 | Male | 39 | 43 925 | 11 689 | 126.46 | Good |
| Case4 | Male | 40 | 44 285 | 12 935 | 120.15 | Good |
| Case5 | Female | 26 | 38 200 | 8111 | 109.66 | Good |
| Case6 | Female | 27 | 38 995 | 10 538 | 103.67 | Excellent |
| Case7 | Female | 54 | 45 045 | 11 346 | 105.87 | Excellent |
| Case8 | Female | 32 | 38 480 | 18 646 | 87.22 | Excellent |
| Case9 | Female | 33 | 37 370 | 17 929 | 88.02 | Excellent |
| Case10 | Female | 35 | 35 070 | 15 663 | 134.82 | Good |
| Case11 | Female | 36 | 34 120 | 11 825 | 147.26 | Excellent |
| Case12 | Female | 63 | 45 875 | 12 569 | 83.74 | Moderate |
| Case13 | Female | 64 | 45 250 | 13 219 | 84.30 | Good |
| Case14 | Female | 38 | 39 495 | 9911 | 128.67 | Good |
| Case15 | Female | 39 | 38 105 | 7527 | 125.40 | Good |
| Case16 | Female | 41 | 38 240 | 6539 | 112.07 | Excellent |
| Case17 | Female | 42 | 36 895 | 3917 | 116.50 | Good |
| Case18 | Male | 33 | 43 880 | 11 475 | 130.13 | Excellent |
| Case19 | Male | 34 | 43 725 | 10 750 | 122.36 | Excellent |
| Case20 | Male | 26 | 39 115 | 10 094 | 104.42 | Excellent |
| Case21 | Male | 27 | 37 945 | 11 575 | 123.99 | Excellent |
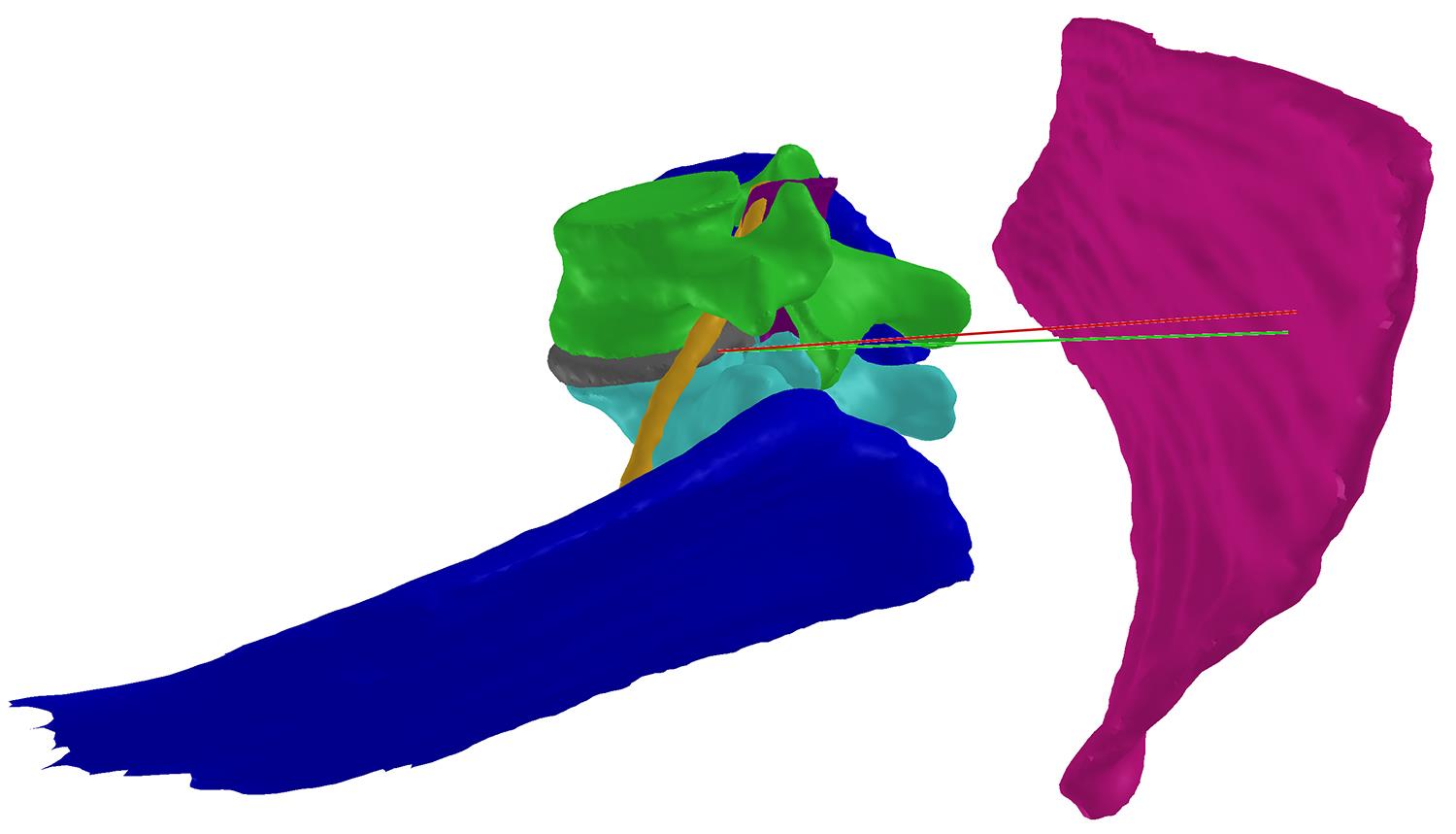
图11 算法规划路径与医师规划路径对比图
Fig.11 Comparison between algorithmically planned paths and doctor-planned paths.
| Soft constraints | Algorithm (ours) | Physician | t/Z | P |
|---|---|---|---|---|
| Diliac(mm) | 9.44±5.10 | 11.88±6.14 | 2.381 | 0.017 |
| DDura(mm) | 17.44±2.38 | 17.23±2.55 | 2.212 | 0.039 |
| DL5(mm) | 8.12±1.66 | 7.20±1.79 | 3.875 | <0.001 |
| DN5(mm) | 6.13±1.84 | 5.66±1.83 | 3.980 | <0.001 |
| DS1(mm) | 0.58±0.17 | 1.25±0.18 | 12.727 | <0.001 |
| Depth(mm) | 113.92±17.44 | 119.51±18.60 | 7.008 | <0.001 |
| AKambin(mm2) | 170.87±59.87 | 148.70±72.83 | 2.868 | 0.004 |
表8 算法与医师规划路径的对比结果
Tab.8 Comparison of the plans by the algorithm and the physician (Mean±SD)
| Soft constraints | Algorithm (ours) | Physician | t/Z | P |
|---|---|---|---|---|
| Diliac(mm) | 9.44±5.10 | 11.88±6.14 | 2.381 | 0.017 |
| DDura(mm) | 17.44±2.38 | 17.23±2.55 | 2.212 | 0.039 |
| DL5(mm) | 8.12±1.66 | 7.20±1.79 | 3.875 | <0.001 |
| DN5(mm) | 6.13±1.84 | 5.66±1.83 | 3.980 | <0.001 |
| DS1(mm) | 0.58±0.17 | 1.25±0.18 | 12.727 | <0.001 |
| Depth(mm) | 113.92±17.44 | 119.51±18.60 | 7.008 | <0.001 |
| AKambin(mm2) | 170.87±59.87 | 148.70±72.83 | 2.868 | 0.004 |
| Soft constraints | Auto segmentation | Manual segmentation | t/Z | P |
|---|---|---|---|---|
| Diliac(mm) | 7.54±5.54 | 9.44±5.10 | 2.958 | 0.008 |
| DDura(mm) | 18.43±2.18 | 17.44±2.38 | 2.071 | 0.052 |
| DL5(mm) | 7.99±1.49 | 8.12±1.66 | 0.535 | 0.599 |
| DN5(mm) | 5.94±1.92 | 6.13±1.84 | 0.678 | 0.498 |
| DS1(mm) | 1.07±0.94 | 0.58±0.17 | 2.311 | 0.021 |
| Depth(mm) | 111.90±16.97 | 113.92±17.44 | 1.477 | 0.140 |
| AKambin(mm2) | 154.62±48.07 | 170.87±59.87 | 2.066 | 0.052 |
表9 自动分割和手动分割数据的算法性能比较
Tab.9 Algorithm performance comparison of auto-segmented and manually segmented data (Mean±SD)
| Soft constraints | Auto segmentation | Manual segmentation | t/Z | P |
|---|---|---|---|---|
| Diliac(mm) | 7.54±5.54 | 9.44±5.10 | 2.958 | 0.008 |
| DDura(mm) | 18.43±2.18 | 17.44±2.38 | 2.071 | 0.052 |
| DL5(mm) | 7.99±1.49 | 8.12±1.66 | 0.535 | 0.599 |
| DN5(mm) | 5.94±1.92 | 6.13±1.84 | 0.678 | 0.498 |
| DS1(mm) | 1.07±0.94 | 0.58±0.17 | 2.311 | 0.021 |
| Depth(mm) | 111.90±16.97 | 113.92±17.44 | 1.477 | 0.140 |
| AKambin(mm2) | 154.62±48.07 | 170.87±59.87 | 2.066 | 0.052 |
| 1 | 周谋望, 岳寿伟, 何成奇, 等. “腰椎间盘突出症的康复治疗” 中国专家共识[J]. 中国康复医学杂志, 2017, 32(2): 129-35. |
| 2 | Ucar D, Duman S, Bayram Y, et al. Extruded disc herniations are experienced earlier by inactive young people in the high-tech gaming era[J]. J Med Life, 2021, 14(3): 402-7. |
| 3 | Deyo RA, Mirza SK. CLINICAL PRACTICE. herniated lumbar intervertebral disk[J]. N Engl J Med, 2016, 374(18): 1763-72. |
| 4 | Martin MD, Boxell CM, Malone DG. Pathophysiology of lumbar disc degeneration: a review of the literature[J]. Neurosurg Focus, 2002, 13(2): E1. |
| 5 | Beyaz SG, Ülgen AM, Kaya B, et al. A novel combination technique: three points of epiduroscopic laser neural decompression and percutaneous laser disc decompression with the Ho: YAG laser in an MSU classification 3AB herniated disc[J]. Pain Pract, 2020, 20(5): 501-9. |
| 6 | Wei WB, Dang SJ, Wei L, et al. Transforaminal epidural steroid injection combined with radio frequency for the treatment of lumbar disc herniation: a 2-year follow-up[J]. BMC Musculoskelet Disord, 2021, 22(1): 347. |
| 7 | 王锁良, 吕建国, 申晓东, 等. 射频热凝靶点消融术在颈腰椎间盘突出症中的应用[J]. 西安交通大学学报(医学版), 2008, 29(2): 236-8. |
| 8 | Wang HW, Huang B, Li CQ, et al. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon’s training level of minimally invasive spine surgery[J]. Clin Neurol Neurosurg, 2013, 115(10): 1987-91. |
| 9 | Ruetten S, Komp M, Godolias G. An extreme lateral access for the surgery of lumbar disc herniations inside the spinal canal using the full-endoscopic uniportal transforaminal approach-technique and prospective results of 463 patients[J]. Spine, 2005, 30(22): 2570-8. |
| 10 | Ju CI. Technical considerations of the transforaminal approach for lumbar disk herniation[J]. World Neurosurg, 2021, 145: 597-611. |
| 11 | Scorza D, El Hadji S, Cortés C, et al. Surgical planning assistance in keyhole and percutaneous surgery: a systematic review[J]. Med Image Anal, 2021, 67: 101820. |
| 12 | Kikinis R, Pieper SD, Vosburgh KG. 3D slicer: a platform for subject-specific image analysis, visualization, and clinical support[M]// Intraoperative Imaging and Image-Guided Therapy. New York: Springer, 2014: 277-89. |
| 13 | Huang Y, Yu LF, Zhang FF. A survey on puncture models and path planning algorithms of bevel-tipped flexible needles[J]. Heliyon, 2024, 10(3): e25002. |
| 14 | Baegert C, Villard C, Schreck P, et al. Multi-criteria trajectory planning for hepatic radiofrequency ablation[J]. Med Image Comput Comput Assist Interv, 2007, 10(Pt 2): 676-84. |
| 15 | Baegert C, Villard C, Schreck P, et al. Trajectory optimization for the planning of percutaneous radiofrequency ablation of hepatic tumors[J]. Comput Aided Surg, 2007, 12(2): 82-90. |
| 16 | Seitel A, Engel M, Sommer CM, et al. Computer-assisted trajectory planning for percutaneous needle insertions[J]. Med Phys, 2011, 38(6): 3246-59. |
| 17 | Li RK, An CY, Wang SX, et al. A heuristic method for rapid and automatic radiofrequency ablation planning of liver tumors[J]. Int J Comput Assist Radiol Surg, 2023, 18(12): 2213-21. |
| 18 | Patil S, Burgner J, Webster RJ 3rd, et al. Needle steering in 3-D via rapid replanning[J]. IEEE Trans Robot, 2014, 30(4): 853-64. |
| 19 | Zhao X, Guo H, Ye D, et al. Comparison of Estimation and Control Methods for Flexible Needle in 2D[C]//东北大学, IEEE新加坡工业电子分会. 第28届中国控制与决策会议论文集(下), 2016: 6. |
| 20 | 赵燕江, 黄 磊, 杜海艳, 等. 基于改进RRT算法的套管柔性针运动规划[J]. 仪器仪表学报, 2017, 38(3): 620-8. |
| 21 | Cai CX, Sun CS, Han Y, et al. Clinical flexible needle puncture path planning based on particle swarm optimization[J]. Comput Methods Programs Biomed, 2020, 193: 105511. |
| 22 | Shahriari N, Georgiadis JR, Oudkerk M, et al. Hybrid control algorithm for flexible needle steering: demonstration in phantom and human cadaver[J]. PLoS One, 2018, 13(12): e0210052. |
| 23 | Vaswani A, Shazeer N, Parmar N, et al. Attention is all you need[EB/OL]. 2017: arXiv: 1706.03762. |
| 24 | Çiçek Ö, Abdulkadir A, Lienkamp SS, et al. 3D U-net: learning dense volumetric segmentation from sparse annotation[C]//International Conference on Medical Image Computing and Computer-Assisted Intervention. Cham: Springer, 2016: 424-32. |
| 25 | Ma HP, Hung YF, Tsai SH, et al. Predictions of the length of lumbar puncture needles[J]. Comput Math Methods Med, 2014, 2014: 732694. |
| 26 | Eun SS, Lee SH, Liu WC, et al. A novel preoperative trajectory evaluation method for L5-S1 transforaminal percutaneous endoscopic lumbar discectomy[J]. Spine J, 2018, 18(7): 1286-91. |
| 27 | Tezuka F, Sakai T, Abe M, et al. Anatomical considerations of the iliac crest on percutaneous endoscopic discectomy using a transforaminal approach[J]. Spine J, 2017, 17(12): 1875-80. |
| 28 | Jones MW, Baerentzen JA, Sramek M. 3D distance fields: a survey of techniques and applications[J]. IEEE Trans Vis Comput Graph, 2006, 12(4): 581-99. |
| 29 | Zhou HY, Guo JS, Zhang YH, et al. nnFormer: volumetric medical image segmentation via a 3D transformer[J]. IEEE Trans Image Process, 2023, 32: 4036-45. |
| 30 | Chen LC, Papandreou G, Schroff F, et al. Rethinking atrous convolution for semantic image segmentation[J/OL]. arXiv E Prints, 2017: arXiv: . |
| 31 | Zhou ZW, Siddiquee MMR, Tajbakhsh N, et al. UNet: redesigning skip connections to exploit multiscale features in image segmentation[J]. IEEE Trans Med Imag, 2020, 39(6): 1856-67. |
| 32 | Diakogiannis FI, Waldner F, Caccetta P, et al. ResUNet-a: a deep learning framework for semantic segmentation of remotely sensed data[J]. ISPRS J Photogramm Remote Sens, 2020, 162: 94-114. |
| 33 | Milletari F, Navab N, Ahmadi SA. V-net: fully convolutional neural networks for volumetric medical image segmentation[C]//2016 Fourth International Conference on 3D Vision (3DV). Stanford, CA, USA. IEEE, 2016: 565-71. |
| 34 | Overley SC, Cho SK, Mehta AI, et al. Navigation and robotics in spinal surgery: where are we now?[J]. Neurosurgery, 2017, 80(3S): S86-99. |
| 35 | 李玉希, 黄浚燊, 刘 婷, 等. 脊柱手术机器人在脊柱外科手术中的应用进展[J]. 机器人外科学杂志: 中英文, 2021, 2(2): 143-50. |
| 36 | Villard C, Baegert C, Schreck P, et al. Optimal trajectories computation within regions of interest for hepatic RFA planning[J]. Med Image Comput Comput Assist Interv, 2005, 8(Pt 2): 49-56. |
| 37 | Liang LB, Cool D, Kakani N, et al. Multiple objective planning for thermal ablation of liver tumors[J]. Int J Comput Assist Radiol Surg, 2020, 15(11): 1775-86. |
| 38 | 刘晓熙, 姜慧研, 骆 敏. 面向肝癌消融术的多约束最优穿刺路径规划算法[J]. 东北大学学报: 自然科学版, 2023, 44(7): 922-30. |
| 39 | Liu YJ. Potential risk of intelligent technologies in clinical orthopedics[J]. Adv Exp Med Biol, 2018, 1093: 281-8. |
| 40 | Zhao L, Pang SM, Chen YF, et al. SpineRegNet: spine Registration Network for volumetric MR and CT image by the joint estimation of an affine-elastic deformation field[J]. Med Image Anal, 2023, 86: 102786. |
| No related articles found! |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||