Journal of Southern Medical University ›› 2024, Vol. 44 ›› Issue (9): 1831-1838.doi: 10.12122/j.issn.1673-4254.2024.09.24
Liping ZHANG1,2( ), Xijuan LIU2, Xiao HU2, Jiali WANG2, Xihe YU2, Guoliang LI2, Haimin YOU2, Qizhou ZHANG2, Haibo ZHANG1()
), Xijuan LIU2, Xiao HU2, Jiali WANG2, Xihe YU2, Guoliang LI2, Haimin YOU2, Qizhou ZHANG2, Haibo ZHANG1()
Received:2023-11-25
Online:2024-09-20
Published:2024-09-30
Contact:
Haibo ZHANG
E-mail:252768046@qq.com;haibozh@gzucm.edu.cn
Liping ZHANG, Xijuan LIU, Xiao HU, Jiali WANG, Xihe YU, Guoliang LI, Haimin YOU, Qizhou ZHANG, Haibo ZHANG. Efficacy and safety of transcatheter arterial chemoembolization followed by hepatic arterial infusion chemotherapy combined with TKI and PD-1 inhibitors as first-line treatment for advanced hepatocellular carcinoma[J]. Journal of Southern Medical University, 2024, 44(9): 1831-1838.
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.j-smu.com/EN/10.12122/j.issn.1673-4254.2024.09.24
| Item | TACE+HAIC+TKI (n=23) | TACE+HAIC+PD-1+TKI (n=47) | P |
|---|---|---|---|
| Gender | 0.207 | ||
| Male | 16 (69.56%) | 39 (82.98%) | |
| Female | 7 (30.44%) | 8 (17.02%) | |
| Age (years) | 63.2 | 53.6 | <0.001 |
| CNLC Stage | <0.001 | ||
| II | 12 (52.17%) | 3 (6.38%) | |
| III | 11 (47.83%) | 44 (93.62%) | |
| Tumor diameter (cm) | 0.216 | ||
| <10 | 20 (86.96%) | 33 (70.21%) | |
| >10 | 3 (13.04%) | 14 (29.79%) | |
| PVTT | 0.042 | ||
| No | 15 (65.22%) | 17 (36.17%) | |
| Yes | 8 (34.78%) | 30 (63.83%) | |
| Extrahpatic M | 0.031 | ||
| >3 | 5 (21.74%) | 23 (48.94%) | |
| 1-3 | 3 (13.04%) | 9 (19.15%) | |
| 0 | 15 (65.22%) | 15 (31.91%) | |
| Hepatitis | 1.000 | ||
| Hepatitis B | 22 (95.65%) | 44 (93.62%) | |
| Hepatitis C | 0 (0.00%) | 1 (2.13%) | |
| No | 1 (4.35%) | 2 (4.26%) | |
| C-P classification | 0.725 | ||
| A | 14 (60.87%) | 25 (53.19%) | |
| B | 9 (39.13%) | 22 (46.81%) | |
| ECOG score | 0.217 | ||
| 0 | 1 (4.35%) | 0 (0.00%) | |
| 1 | 12 (52.17%) | 31 (65.96%) | |
| 2 | 10 (43.48%) | 16 (34.04%) | |
| KPS score | 0.551 | ||
| 60 | 0 (0.00%) | 1 (2.13%) | |
| 70 | 3 (13.04%) | 7 (14.89%) | |
| 80 | 14 (60.87%) | 33 (70.21%) | |
| 90 | 6 (26.09%) | 6 (12.77%) | |
| TACE/HAIC cycle | 3.00 (2.0; 4.0) | 3.00 (2.0; 4.0) | 0.948 |
Tab.1 Clinical characteristics of the patients with advanced HCC in the two groups [n (%)]
| Item | TACE+HAIC+TKI (n=23) | TACE+HAIC+PD-1+TKI (n=47) | P |
|---|---|---|---|
| Gender | 0.207 | ||
| Male | 16 (69.56%) | 39 (82.98%) | |
| Female | 7 (30.44%) | 8 (17.02%) | |
| Age (years) | 63.2 | 53.6 | <0.001 |
| CNLC Stage | <0.001 | ||
| II | 12 (52.17%) | 3 (6.38%) | |
| III | 11 (47.83%) | 44 (93.62%) | |
| Tumor diameter (cm) | 0.216 | ||
| <10 | 20 (86.96%) | 33 (70.21%) | |
| >10 | 3 (13.04%) | 14 (29.79%) | |
| PVTT | 0.042 | ||
| No | 15 (65.22%) | 17 (36.17%) | |
| Yes | 8 (34.78%) | 30 (63.83%) | |
| Extrahpatic M | 0.031 | ||
| >3 | 5 (21.74%) | 23 (48.94%) | |
| 1-3 | 3 (13.04%) | 9 (19.15%) | |
| 0 | 15 (65.22%) | 15 (31.91%) | |
| Hepatitis | 1.000 | ||
| Hepatitis B | 22 (95.65%) | 44 (93.62%) | |
| Hepatitis C | 0 (0.00%) | 1 (2.13%) | |
| No | 1 (4.35%) | 2 (4.26%) | |
| C-P classification | 0.725 | ||
| A | 14 (60.87%) | 25 (53.19%) | |
| B | 9 (39.13%) | 22 (46.81%) | |
| ECOG score | 0.217 | ||
| 0 | 1 (4.35%) | 0 (0.00%) | |
| 1 | 12 (52.17%) | 31 (65.96%) | |
| 2 | 10 (43.48%) | 16 (34.04%) | |
| KPS score | 0.551 | ||
| 60 | 0 (0.00%) | 1 (2.13%) | |
| 70 | 3 (13.04%) | 7 (14.89%) | |
| 80 | 14 (60.87%) | 33 (70.21%) | |
| 90 | 6 (26.09%) | 6 (12.77%) | |
| TACE/HAIC cycle | 3.00 (2.0; 4.0) | 3.00 (2.0; 4.0) | 0.948 |
| Group | ORR | DCR | P |
|---|---|---|---|
| TACE+HAIC+TKI (n=23) | 60.87% (14/23) | 95.65% (22/23) | 0.031 |
| TACE+HAIC+PD-1+TKI (n=47) | 36.17% (17/47) | 93.62% (44/47) | 0.068 |
Tab.2 Objective remission rates (ORR) and disease control rates (DCR) in the two groups
| Group | ORR | DCR | P |
|---|---|---|---|
| TACE+HAIC+TKI (n=23) | 60.87% (14/23) | 95.65% (22/23) | 0.031 |
| TACE+HAIC+PD-1+TKI (n=47) | 36.17% (17/47) | 93.62% (44/47) | 0.068 |
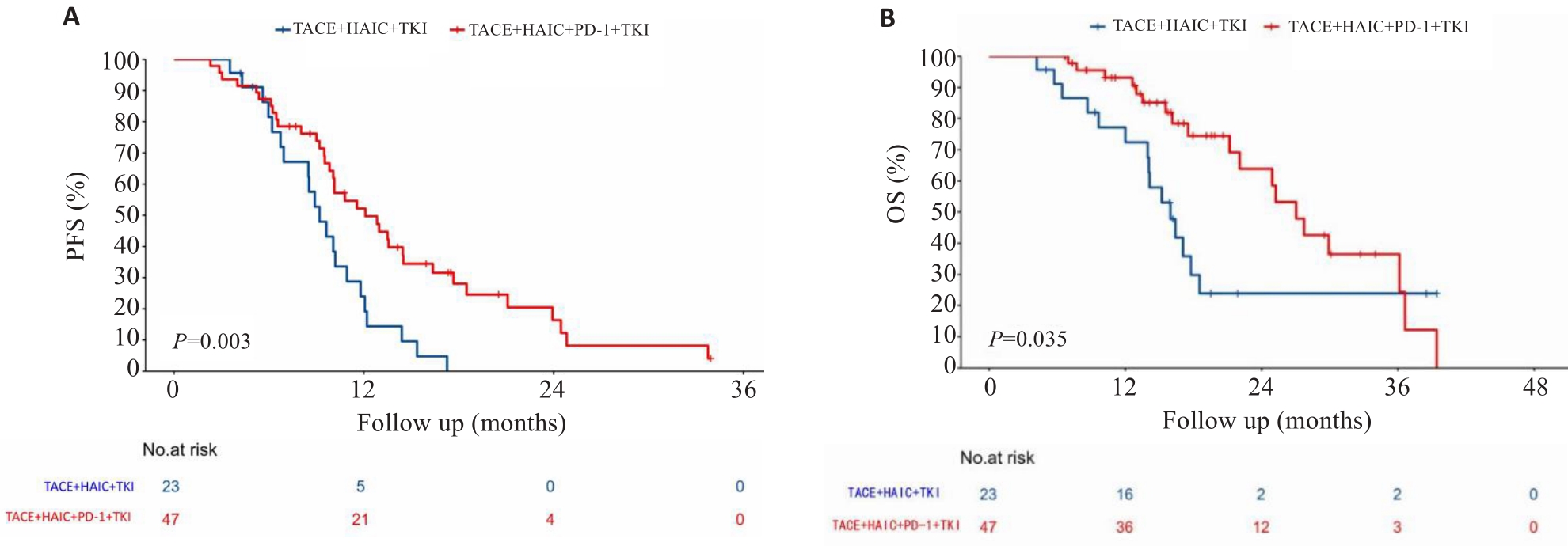
Fig.1 Kaplan-Meier survival analysis of the HCC patients in the two groups. A: Progression-free survival (PFS). B: Overall survival (OS).
| Group | 1 year-PFS (95% CI) | 2 years-PFS (95% CI) |
|---|---|---|
| TACE+HAIC+TKI (n=23) | 24.0% (11.2%, 51.4%) | NA |
| TACE+HAIC+PD-1+TKI (n=47) | 52.2% (39.2%, 69.5%) | 16.4% (7.3%, 36.7%) |
Tab.3 1- and 2-year PFS of advanced HCC patients in the two groups
| Group | 1 year-PFS (95% CI) | 2 years-PFS (95% CI) |
|---|---|---|
| TACE+HAIC+TKI (n=23) | 24.0% (11.2%, 51.4%) | NA |
| TACE+HAIC+PD-1+TKI (n=47) | 52.2% (39.2%, 69.5%) | 16.4% (7.3%, 36.7%) |
| Group | 1year-OS (95% CI) | 2years-OS (95% CI) | 3years-OS (95% CI) |
|---|---|---|---|
| TACE+HAIC+TKI (n=23) | 72.3% (55.7%, 93.9%) | 23.9% (10.4%, 54.6%) | 23.9% (10.4%, 54.6%) |
| TACE+HAIC+PD-1+TKI (n=47) | 93.1% (85.9%, 100%) | 63.8% (47.6%, 85.6%) | 36.5% (20.4%, 65.2%) |
Tab.4 1-, 2-, and 3-year OS of advanced HCC patients in the two groups
| Group | 1year-OS (95% CI) | 2years-OS (95% CI) | 3years-OS (95% CI) |
|---|---|---|---|
| TACE+HAIC+TKI (n=23) | 72.3% (55.7%, 93.9%) | 23.9% (10.4%, 54.6%) | 23.9% (10.4%, 54.6%) |
| TACE+HAIC+PD-1+TKI (n=47) | 93.1% (85.9%, 100%) | 63.8% (47.6%, 85.6%) | 36.5% (20.4%, 65.2%) |
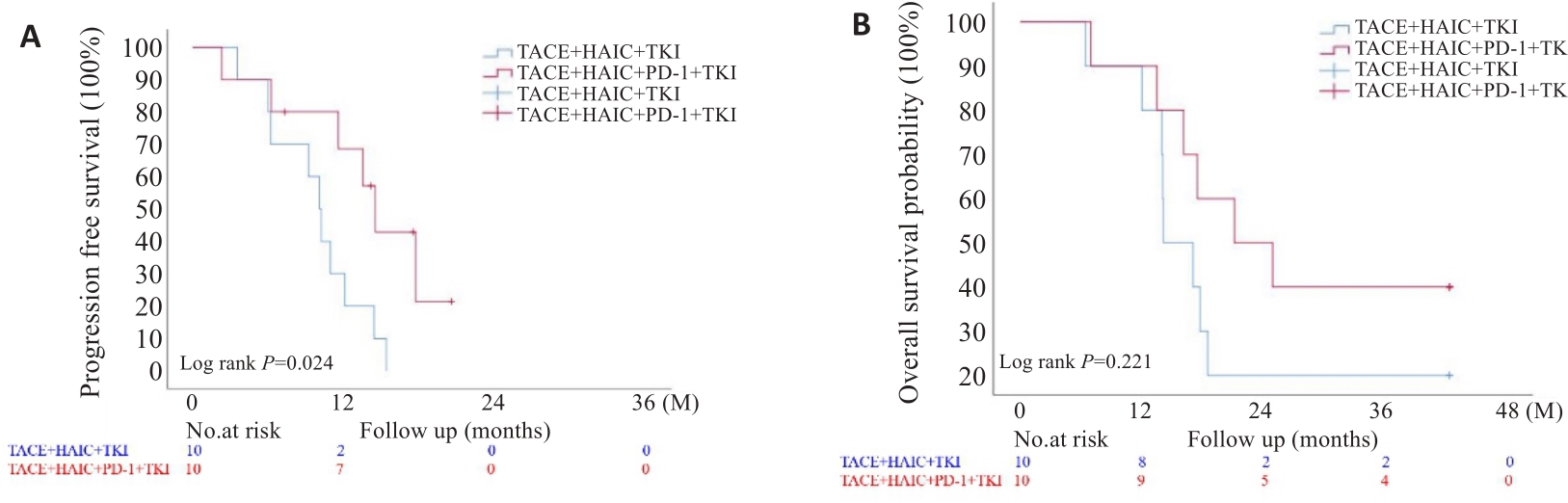
Fig.2 Kaplan-Meier survival analysis of the two groups of HCC patients after propensity score matching analysis. A: PFS outcome; B: OS outcome.
| Item | P | HR | 95% CI | |
|---|---|---|---|---|
| Lower limit | Upper limit | |||
| Treatment regime | 0.022 | 0.001 | 0.001 | 0.366 |
| Gender | 0.167 | 11.658 | 0.357 | 380.361 |
| Age(years) | 0.005 | 0.678 | 0.518 | 0.888 |
| Tumor diameter | 0.039 | 0.002 | 0.001 | 0.731 |
| PVTT | 0.325 | 6.957 | 0.146 | 331.837 |
| Hepatitis background | 0.966 | 650095 | 0.001 | 780.361 |
| Chlid-Pugh classification | 0.877 | 0.664 | 0.004 | 120.909 |
| ECOG score (0) | 0.424 | 0.111 | 0.001 | 24.453 |
| KPS score (60) | 0.034 | |||
| 70 | 0.003 | 0.001 | 0.001 | 0.001 |
| 80 | 0.005 | 0.001 | 0.001 | 0.002 |
| 90 | 0.006 | 0.001 | 0.001 | 0.004 |
| Surgery | 0.278 | 0.016 | 0.001 | 28.466 |
| TACE/HAIC cycles | 0.031 | 3.191 | 1.115 | 9.132 |
Tab.5 Multivariate Cox regression analysis of survival in patients with advanced HCC
| Item | P | HR | 95% CI | |
|---|---|---|---|---|
| Lower limit | Upper limit | |||
| Treatment regime | 0.022 | 0.001 | 0.001 | 0.366 |
| Gender | 0.167 | 11.658 | 0.357 | 380.361 |
| Age(years) | 0.005 | 0.678 | 0.518 | 0.888 |
| Tumor diameter | 0.039 | 0.002 | 0.001 | 0.731 |
| PVTT | 0.325 | 6.957 | 0.146 | 331.837 |
| Hepatitis background | 0.966 | 650095 | 0.001 | 780.361 |
| Chlid-Pugh classification | 0.877 | 0.664 | 0.004 | 120.909 |
| ECOG score (0) | 0.424 | 0.111 | 0.001 | 24.453 |
| KPS score (60) | 0.034 | |||
| 70 | 0.003 | 0.001 | 0.001 | 0.001 |
| 80 | 0.005 | 0.001 | 0.001 | 0.002 |
| 90 | 0.006 | 0.001 | 0.001 | 0.004 |
| Surgery | 0.278 | 0.016 | 0.001 | 28.466 |
| TACE/HAIC cycles | 0.031 | 3.191 | 1.115 | 9.132 |
| Item | TACE+HAIC+TKI (n=23) | TACE+HAIC+PD-1+TKI (n=47) | P |
|---|---|---|---|
| Any TRAEs | 1.000 | ||
| No | 0 (0.00%) | 1 (2.13%) | |
| Yes | 23 (100.00%) | 46 (97.87%) | |
| Hematologic TRAEs | 1.000 | ||
| No | 4 (17.39%) | 10 (21.28%) | |
| Yes | 19 (82.61%) | 37 (78.72%) | |
| Grade3-4 granulocytopenia | 1.000 | ||
| No | 14 (60.87%) | 29 (61.70%) | |
| Yes | 9 (39.13%) | 18 (38.30%) | |
| Grade3-4 thrombocytopenia | 1.000 | ||
| No | 20 (86.96%) | 39 (82.98%) | |
| Yes | 3 (13.04%) | 8 (17.02%) | |
| Grade3-4 anaemia | 1.000 | ||
| No | 23 (100.00%) | 46 (97.87%) | |
| Yes | 0 (0.00%) | 1 (2.13%) | |
| Grade3-4febrile neutropenia | 0.361 | ||
| No | 20 (86.96%) | 36 (76.60%) | |
| Yes | 3 (13.04%) | 11 (23.40%) | |
| Digestive system TRAEs | 0.656 | ||
| No | 1 (4.35%) | 5 (10.64%) | |
| Yes | 22 (95.65%) | 42 (89.36%) | |
| Grade3-4 nausea and vomiting | 0.676 | ||
| No | 20 (86.96%) | 43 (91.49%) | |
| Yes | 3 (13.04%) | 4 (8.51%) | |
| Grade3-4 Diarrhea | 1.000 | ||
| No | 22 (95.65%) | 43 (91.49%) | |
| Yes | 1 (4.35%) | 4 (8.51%) | |
| Abnormal liver function | 0.143 | ||
| No | 5 (21.74%) | 4 (8.51%) | |
| Yes | 18 (78.26%) | 43 (91.49%) | |
| Grade3-4 Increased bilirubin | 1.000 | ||
| No | 21 (91.30%) | 42 (89.36%) | |
| Yes | 2 (8.70%) | 5 (10.64%) | |
| Grade3-4 Increased alanine aminotransferase | 0.583 | ||
| No | 16 (69.57%) | 28 (59.57%) | |
| Yes | 7 (30.43%) | 19 (40.43%) | |
| Skin toxicity | 0.304 | ||
| No | 15 (65.22%) | 23 (48.94%) | |
| Yes | 8 (34.78%) | 24 (51.06%) | |
| Grade3-4 hand-foot syndrome | 0.329 | ||
| No | 22 (95.65%) | 47 (100.00%) | |
| Yes | 1 (4.35%) | 0 (0.00%) | |
| Grade3-4 rash | 1.000 | ||
| No | 22 (95.65%) | 44 (93.62%) | |
| Yes | 1 (4.35%) | 3 (6.38%) | |
| Hypertension | 0.387 | ||
| No | 13 (56.52%) | 33 (70.21%) | |
| Yes | 10 (43.48%) | 14 (29.79%) | |
| Grade3-4 hypertension | 1.000 | ||
| No | 23 (100.00%) | 46 (97.87%) | |
| Yes | 0 (0.00%) | 1 (2.13%) | |
| Protenuria | 0.025 | ||
| No | 23 (100.00%) | 37 (78.72%) | |
| Yes | 0 (0.00%) | 10 (21.28%) | |
| Grade3-4 Protenuria | 0.119 | ||
| No | 23 (100.00%) | 47 (100.00%) | |
| Yes | 0 (0.00%) | 0 (0.00%) | |
| Hypothyroidism | 1.000 | ||
| No | 21 (91.30%) | 34 (72.34%) | |
| Yes | 2 (8.70%) | 13 (27.66%) | |
| Treatment related deaths | 0.970 | ||
| No | 23 (100.00%) | 46 (97.87%) | |
| Yes | 0 (0.00%) | 1 (2.13%) |
Tab.6 Incidences of treatment-related adverse events in the two groups
| Item | TACE+HAIC+TKI (n=23) | TACE+HAIC+PD-1+TKI (n=47) | P |
|---|---|---|---|
| Any TRAEs | 1.000 | ||
| No | 0 (0.00%) | 1 (2.13%) | |
| Yes | 23 (100.00%) | 46 (97.87%) | |
| Hematologic TRAEs | 1.000 | ||
| No | 4 (17.39%) | 10 (21.28%) | |
| Yes | 19 (82.61%) | 37 (78.72%) | |
| Grade3-4 granulocytopenia | 1.000 | ||
| No | 14 (60.87%) | 29 (61.70%) | |
| Yes | 9 (39.13%) | 18 (38.30%) | |
| Grade3-4 thrombocytopenia | 1.000 | ||
| No | 20 (86.96%) | 39 (82.98%) | |
| Yes | 3 (13.04%) | 8 (17.02%) | |
| Grade3-4 anaemia | 1.000 | ||
| No | 23 (100.00%) | 46 (97.87%) | |
| Yes | 0 (0.00%) | 1 (2.13%) | |
| Grade3-4febrile neutropenia | 0.361 | ||
| No | 20 (86.96%) | 36 (76.60%) | |
| Yes | 3 (13.04%) | 11 (23.40%) | |
| Digestive system TRAEs | 0.656 | ||
| No | 1 (4.35%) | 5 (10.64%) | |
| Yes | 22 (95.65%) | 42 (89.36%) | |
| Grade3-4 nausea and vomiting | 0.676 | ||
| No | 20 (86.96%) | 43 (91.49%) | |
| Yes | 3 (13.04%) | 4 (8.51%) | |
| Grade3-4 Diarrhea | 1.000 | ||
| No | 22 (95.65%) | 43 (91.49%) | |
| Yes | 1 (4.35%) | 4 (8.51%) | |
| Abnormal liver function | 0.143 | ||
| No | 5 (21.74%) | 4 (8.51%) | |
| Yes | 18 (78.26%) | 43 (91.49%) | |
| Grade3-4 Increased bilirubin | 1.000 | ||
| No | 21 (91.30%) | 42 (89.36%) | |
| Yes | 2 (8.70%) | 5 (10.64%) | |
| Grade3-4 Increased alanine aminotransferase | 0.583 | ||
| No | 16 (69.57%) | 28 (59.57%) | |
| Yes | 7 (30.43%) | 19 (40.43%) | |
| Skin toxicity | 0.304 | ||
| No | 15 (65.22%) | 23 (48.94%) | |
| Yes | 8 (34.78%) | 24 (51.06%) | |
| Grade3-4 hand-foot syndrome | 0.329 | ||
| No | 22 (95.65%) | 47 (100.00%) | |
| Yes | 1 (4.35%) | 0 (0.00%) | |
| Grade3-4 rash | 1.000 | ||
| No | 22 (95.65%) | 44 (93.62%) | |
| Yes | 1 (4.35%) | 3 (6.38%) | |
| Hypertension | 0.387 | ||
| No | 13 (56.52%) | 33 (70.21%) | |
| Yes | 10 (43.48%) | 14 (29.79%) | |
| Grade3-4 hypertension | 1.000 | ||
| No | 23 (100.00%) | 46 (97.87%) | |
| Yes | 0 (0.00%) | 1 (2.13%) | |
| Protenuria | 0.025 | ||
| No | 23 (100.00%) | 37 (78.72%) | |
| Yes | 0 (0.00%) | 10 (21.28%) | |
| Grade3-4 Protenuria | 0.119 | ||
| No | 23 (100.00%) | 47 (100.00%) | |
| Yes | 0 (0.00%) | 0 (0.00%) | |
| Hypothyroidism | 1.000 | ||
| No | 21 (91.30%) | 34 (72.34%) | |
| Yes | 2 (8.70%) | 13 (27.66%) | |
| Treatment related deaths | 0.970 | ||
| No | 23 (100.00%) | 46 (97.87%) | |
| Yes | 0 (0.00%) | 1 (2.13%) |
| 1 | Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012[J]. CA A Cancer J Clin, 2015, 65(2): 87-108. |
| 2 | Zhou MG, Wang HD, Zeng XY, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2019, 394(10204): 1145-58. |
| 3 | World Health Organization. GLOBOCAN 2020[EB/OL]. [2023-06-05]. . |
| 4 | 刘庆拿, 孟祥涛, 李忠超, 等. TACE辅助外科手术治疗原发性肝癌临床效果观察[J]. 山东医药, 2016, 56(48): 87-9. |
| 5 | Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma[J]. N Engl J Med, 2008, 359(4): 378-90. |
| 6 | Cheng AL, Kang YK, Chen ZD, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific Region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial[J]. Lancet Oncol, 2009, 10(1): 25-34. |
| 7 | Kudo M, Finn RS, Qin SK, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial[J]. Lancet, 2018, 391(10126): 1163-73. |
| 8 | Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1)[J]. Eur J Cancer, 2009, 45(2): 228-47. |
| 9 | Jia ZZ, Jiang GM, Feng YL. Serum HIF-1α and VEGF levels pre- and post-TACE in patients with primary liver cancer[J]. Chin Med Sci J, 2011, 26(3): 158-62. |
| 10 | Huynh KN, Rao S, Roth B, et al. Targeting hypoxia-inducible factor-1α for the management of hepatocellular carcinoma[J]. Cancers, 2023, 15(10): 2738. |
| 11 | Rimassa L, Finn RS, Sangro B. Combination immunotherapy for hepatocellular carcinoma[J]. J Hepatol, 2023, 79(2): 506-15. |
| 12 | Finn RS, Qin SK, Ikeda M, et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma[J]. N Engl J Med, 2020, 382(20): 1894-905. |
| 13 | Ren ZG, Xu JM, Bai YX, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2-3 study[J]. Lancet Oncol, 2021, 22(7): 977-90. |
| 14 | Finn RS, Ikeda M, Zhu AX, et al. Phase ib study of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma[J]. J Clin Oncol, 2020, 38(26): 2960-70. |
| 15 | Fan WZ, Zhu BW, Yue SF, et al. Idarubicin-Loaded DEB-TACE plus Lenvatinib versus Lenvatinib for patients with advanced hepatocellular carcinoma: a propensity score-matching analysis[J]. Cancer Med, 2023, 12(1): 61-72. |
| 16 | Guo WB, Chen S, Wu ZQ, et al. Efficacy and safety of transarterial chemoembolization combined with anlotinib for unresectable hepatocellular carcinoma: a retrospective study[J]. Technol Cancer Res Treat, 2020, 19: 153303382096558. |
| 17 | Zhang XP, Wang K, Wang M, et al. Transarterial chemoembolization (TACE) combined with sorafenib versus TACE for hepatocellular carcinoma with portal vein tumor thrombus: a systematic review and meta-analysis[J]. Oncotarget, 2017, 8(17): 29416-27. |
| 18 | Zhang ZZ, Wu YF, Zheng TH, et al. Efficacy of transarterial chemoembolization combined with molecular targeted agents for unresectable hepatocellular carcinoma: a network meta-analysis[J]. Cancers, 2022, 14(15): 3710. |
| 19 | Zhang TQ, Geng ZJ, Zuo MX, et al. Camrelizumab (a PD-1 inhibitor) plus apatinib (an VEGFR-2 inhibitor) and hepatic artery infusion chemotherapy for hepatocellular carcinoma in Barcelona Clinic Liver Cancer stage C (TRIPLET): a phase II study[J]. Signal Transduct Target Ther, 2023, 8: 413. |
| 20 | Yang F, Yang J, Xiang W, et al. Safety and efficacy of transarterial chemoembolization combined with immune checkpoint inhibitors and tyrosine kinase inhibitors for hepatocellular carcinoma[J]. Front Oncol, 2021, 11: 657512. |
| 21 | He MK, Liang RB, Zhao Y, et al. Lenvatinib, toripalimab, plus hepatic arterial infusion chemotherapy versus lenvatinib alone for advanced hepatocellular carcinoma[J]. Ther Adv Med Oncol, 2021, 13: 17588359211002720. |
| 22 | Huang JT, Zhong BY, Jiang N, et al. Transarterial chemoembolization combined with immune checkpoint inhibitors plus tyrosine kinase inhibitors versus immune checkpoint inhibitors plus tyrosine kinase inhibitors for advanced hepatocellular carcinoma[J]. J Hepatocell Carcinoma, 2022, 9: 1217-28. |
| 23 | He MK, Li QJ, Zou RH, et al. Sorafenib plus hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin vs sorafenib alone for hepatocellular carcinoma with portal vein invasion: a randomized clinical trial[J]. JAMA Oncol, 2019, 5(7): 953-60. |
| 24 | Yuan YC, He W, Yang ZW, et al. TACE-HAIC combined with targeted therapy and immunotherapy versus TACE alone for hepatocellular carcinoma with portal vein tumour thrombus: a propensity score matching study[J]. Int J Surg, 2023, 109(5): 1222-30. |
| 25 | Huang ZJ, Wu ZY, Zhang LD, et al. The safety and efficacy of TACE combined with HAIC, PD-1 inhibitors, and tyrosine kinase inhibitors for unresectable hepatocellular carcinoma: a retrospective study[J]. Front Oncol, 2024, 14: 1298122. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||