南方医科大学学报 ›› 2026, Vol. 46 ›› Issue (1): 104-112.doi: 10.12122/j.issn.1673-4254.2026.01.11
安建雄1,2,3( ), 迟智佳3, 赵彩群3, 李永祥3, 王若国3, 胡亚楠1,2()
), 迟智佳3, 赵彩群3, 李永祥3, 王若国3, 胡亚楠1,2()
收稿日期:2025-07-15
出版日期:2026-01-20
发布日期:2026-01-16
通讯作者:
胡亚楠
E-mail:anjianxiong@yeah.net;huyanan1998@yeah.net
作者简介:安建雄,教授,博士生导师,E-mail: anjianxiong@yeah.net
基金资助:
Jianxiong AN1,2,3(), Zhijia CHI3, Caiqun ZHAO3, Yongxiang LI3, Ruoguo WANG3, Yanan HU1,2()
Received:2025-07-15
Online:2026-01-20
Published:2026-01-16
Contact:
Yanan HU
E-mail:anjianxiong@yeah.net;huyanan1998@yeah.net
摘要:
目的 比较多次电刺激下显著延长癫痫波发作的超级电休克(super ECT)对难治性抑郁的治疗疗效。 方法 基于人群的队列研究纳入2024年12月~2025年6月接受super ECT的难治性抑郁患者292例。根据一次super ECT中电击次数分为3组:E1组为一次ECT过程电击1次(n=88),E2组为一次ECT过程电击2次(n=89),E3组为一次ECT过程电击3次(n=39)。分析基线抑郁、焦虑和失眠量表评分之间的相关性。首次疗程后第1、3、6个月利用汉密尔顿抑郁量表-17(HAMD-17)评估抑郁症状,基于减分率比较3组治疗缓解率和反应率。比较6个月内治疗次数,再住院率和不良反应发生率。分析首次super ECT治疗时的脑电图(EEG)癫痫波发作持续时间。 结果 E1组74例(84.09%)、E2组76例(76.40%)、E3组32例(82.05%)患者在super ECT后6个月内达到缓解。在6个月内super ECT治疗疗程在E1组为2.13±1.44次,E2组为2.23±2.01次,E3组为2.41±2.15次。基线HAMA、HAMD-17和PSQI评分相关(P<0.001)。第1次癫痫波发作时间在E1组显著高于E2和E3组(P<0.001)。E2组3个月和6个月的再住院率高于E1组(P=0.012、0.026)。短期不良反应包括发热、头痛/头晕、全身痛和口干。 结论 super ECT作为该领域的技术创新方法在>180 s的发作时间下具备临床安全性和有效性。一次麻醉下电击次数对治疗效果无明显影响。
安建雄, 迟智佳, 赵彩群, 李永祥, 王若国, 胡亚楠. 超级电休克在难治性抑郁中应用的临床研究:一项回顾性研究[J]. 南方医科大学学报, 2026, 46(1): 104-112.
Jianxiong AN, Zhijia CHI, Caiqun ZHAO, Yongxiang LI, Ruoguo WANG, Yanan HU. Efficacy and safety of super electroconvulsive therapy for treatment-resistant depression: a retrospective analysis of 292 cases[J]. Journal of Southern Medical University, 2026, 46(1): 104-112.
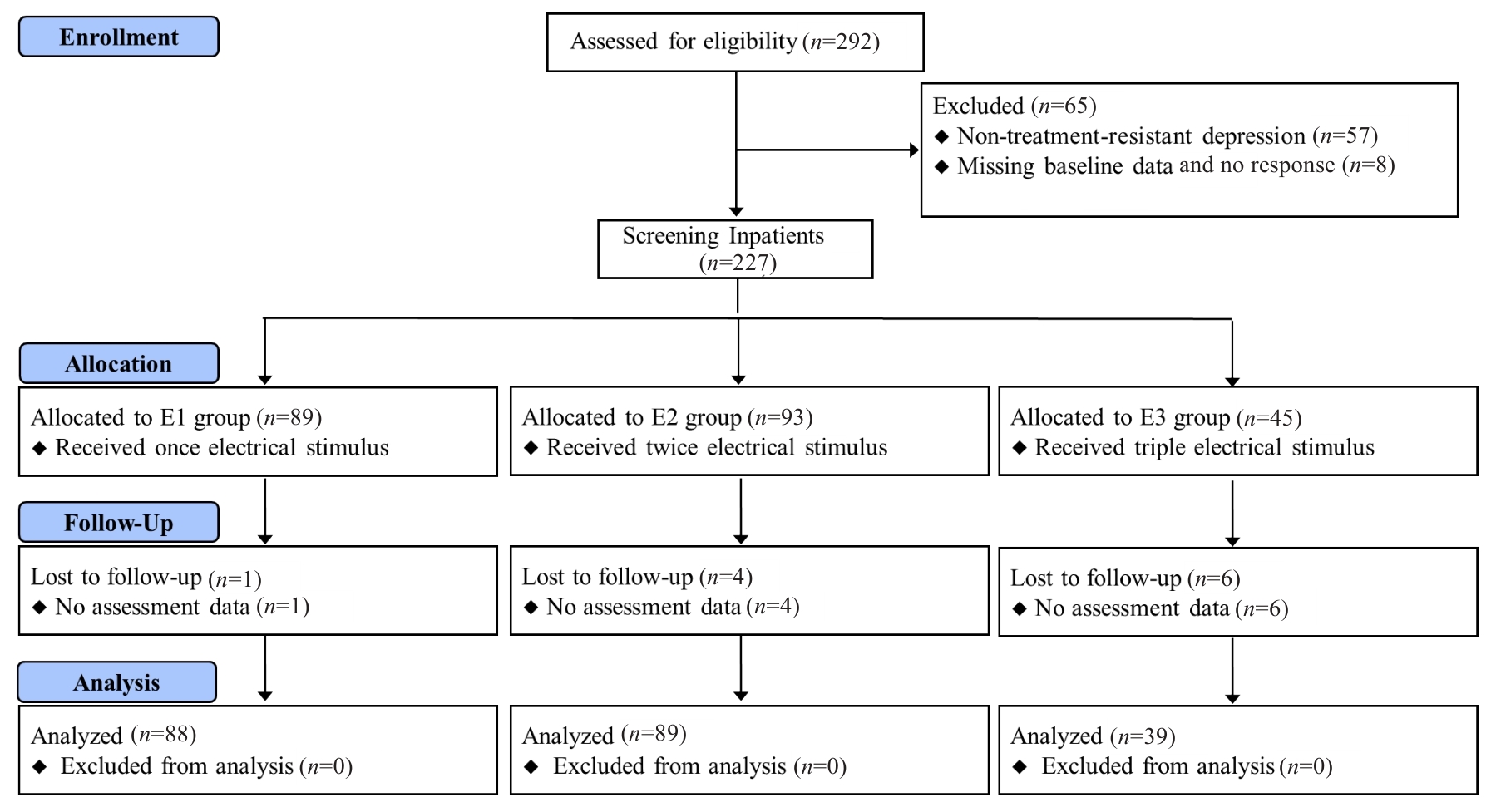
图1 研究流程图
Fig.1 Flow chart of the study.
| Index | E1 (n=88) | E2 (n=89) | E3 (n=39) | P |
|---|---|---|---|---|
| Age (year, Mean±SD) | 27.97±12.83 | 30.43±10.48 | 27.84±12.02 | 0.299 |
Gender [n (%)] Male Female | 43 (48.31) 45 (51.14) | 54 (60.67) 35 (39.33) | 18 (46.15) 21 (53.85) | 0.469 0.513 |
| BMI (kg/m2, Mean±SD) | 28.23±5.35 | 29.23±8.22 | 27.23±7.46 | 0.423 |
Education [n (%)] None ≤6 years >6 years | 13 (14.77) 10 (11.36) 65 (73.86) | 11 (12.36) 18 (20.22) 60 (67.42) | 3 (7.69) 7 (17.95) 29 (74.36) | 0.348 0.472 0.621 |
Medications [n (%)] Antidepressant Sleep medicine | 88 (100) 67 (76.14) | 89 (100) 70 (78.65) | 38 (97.43) 31 (79.48) | 0.989 0.863 |
Suicide attempt [n (%)] Within 1 year No | 62 (70.45) 26 (29.55) | 54 (60.67) 35 (39.33) | 30 (76.92) 9 (23.08) | 0.437 0.265 |
Diagnosis [n (%)] Without psychotic features With psychotic features | 56 (63.64) 32 (36.36) | 61 (68.54) 28 (31.46) | 27 (69.23) 12 (30.77) | 0.652 0.537 |
Anesthesia induction (Mean±SD) Scopolamine (mg) Propofol (mg) Remifentanil (μg) | 0.32±0.07 52.21±5.15 198.31±22.22 | 0.30±0.08 55.34±21.45 202.26±24.14 | 0.30±0.09 51.67±4.49 200.26±24.97 | 0.831 0.243 0.529 |
| Duration between propofol and electric stimulus (min) | 12.11±1.53 | 11.88±1.71 | 12.18±1.75 | 0.522 |
表1 3组一般资料
Tab.1 General characteristics of the patients in the 3 groups
| Index | E1 (n=88) | E2 (n=89) | E3 (n=39) | P |
|---|---|---|---|---|
| Age (year, Mean±SD) | 27.97±12.83 | 30.43±10.48 | 27.84±12.02 | 0.299 |
Gender [n (%)] Male Female | 43 (48.31) 45 (51.14) | 54 (60.67) 35 (39.33) | 18 (46.15) 21 (53.85) | 0.469 0.513 |
| BMI (kg/m2, Mean±SD) | 28.23±5.35 | 29.23±8.22 | 27.23±7.46 | 0.423 |
Education [n (%)] None ≤6 years >6 years | 13 (14.77) 10 (11.36) 65 (73.86) | 11 (12.36) 18 (20.22) 60 (67.42) | 3 (7.69) 7 (17.95) 29 (74.36) | 0.348 0.472 0.621 |
Medications [n (%)] Antidepressant Sleep medicine | 88 (100) 67 (76.14) | 89 (100) 70 (78.65) | 38 (97.43) 31 (79.48) | 0.989 0.863 |
Suicide attempt [n (%)] Within 1 year No | 62 (70.45) 26 (29.55) | 54 (60.67) 35 (39.33) | 30 (76.92) 9 (23.08) | 0.437 0.265 |
Diagnosis [n (%)] Without psychotic features With psychotic features | 56 (63.64) 32 (36.36) | 61 (68.54) 28 (31.46) | 27 (69.23) 12 (30.77) | 0.652 0.537 |
Anesthesia induction (Mean±SD) Scopolamine (mg) Propofol (mg) Remifentanil (μg) | 0.32±0.07 52.21±5.15 198.31±22.22 | 0.30±0.08 55.34±21.45 202.26±24.14 | 0.30±0.09 51.67±4.49 200.26±24.97 | 0.831 0.243 0.529 |
| Duration between propofol and electric stimulus (min) | 12.11±1.53 | 11.88±1.71 | 12.18±1.75 | 0.522 |
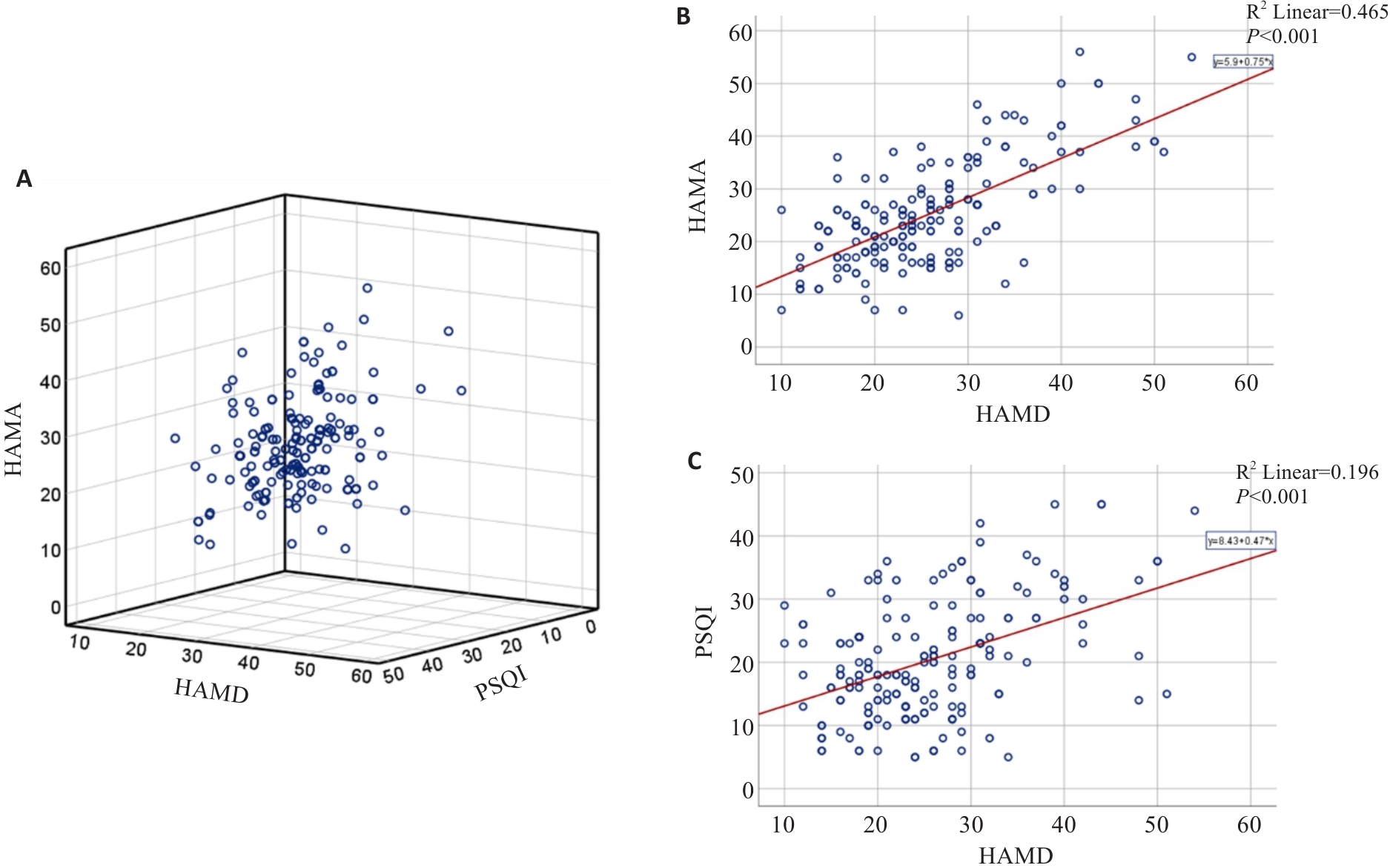
图2 基于HAMA、HAMD-17及PSQI基线评分评估其相关性
Fig.2 Correlation among HAMA, HAMD-17, and PSQI scores of the patients at baseline. A: 3-D scatterplot of the relation among HAMA, HAMD-17 and PSQI scores. B: Correlation between HAMA and HAMD-17 scores. C: Correlation between PSQI and HAMD-17 scores.
| Variables | E1 (n=88) | E2 (n=89) | E3 (n=39) | P |
|---|---|---|---|---|
EEG seizure duration (s) Total First Second Third | 235.3±123.79 235.3±123.79† - - | 208.76±72.99 77.85±27.50* 112.26±62.01 - | 231.85±93.34 50.56±22.99* 64.33±13.20 115.15±75.08 | 0.171 <0.001 0.185 - |
| Super ECT sessions | 2.13±1.44 | 2.23±2.01 | 2.41±2.15 | 0.759 |
Race of hospitalizations [n(%)] 1 month 3 months 6 months | 44 (50.00) 8 (9.09) 13 (14.77) 19 (21.59) | 43 (48.31) 14 (15.73) 28 (31.46)* 32 (35.96)* | 17 (43.59) 7 (17.95) 10 (25.64) 11 (28.21) | 0.383 0.470 0.012 0.026 |
表2 癫痫波发作时间分析和治疗情况
Tab.2 Seizure duration analysis and treatment conditions
| Variables | E1 (n=88) | E2 (n=89) | E3 (n=39) | P |
|---|---|---|---|---|
EEG seizure duration (s) Total First Second Third | 235.3±123.79 235.3±123.79† - - | 208.76±72.99 77.85±27.50* 112.26±62.01 - | 231.85±93.34 50.56±22.99* 64.33±13.20 115.15±75.08 | 0.171 <0.001 0.185 - |
| Super ECT sessions | 2.13±1.44 | 2.23±2.01 | 2.41±2.15 | 0.759 |
Race of hospitalizations [n(%)] 1 month 3 months 6 months | 44 (50.00) 8 (9.09) 13 (14.77) 19 (21.59) | 43 (48.31) 14 (15.73) 28 (31.46)* 32 (35.96)* | 17 (43.59) 7 (17.95) 10 (25.64) 11 (28.21) | 0.383 0.470 0.012 0.026 |
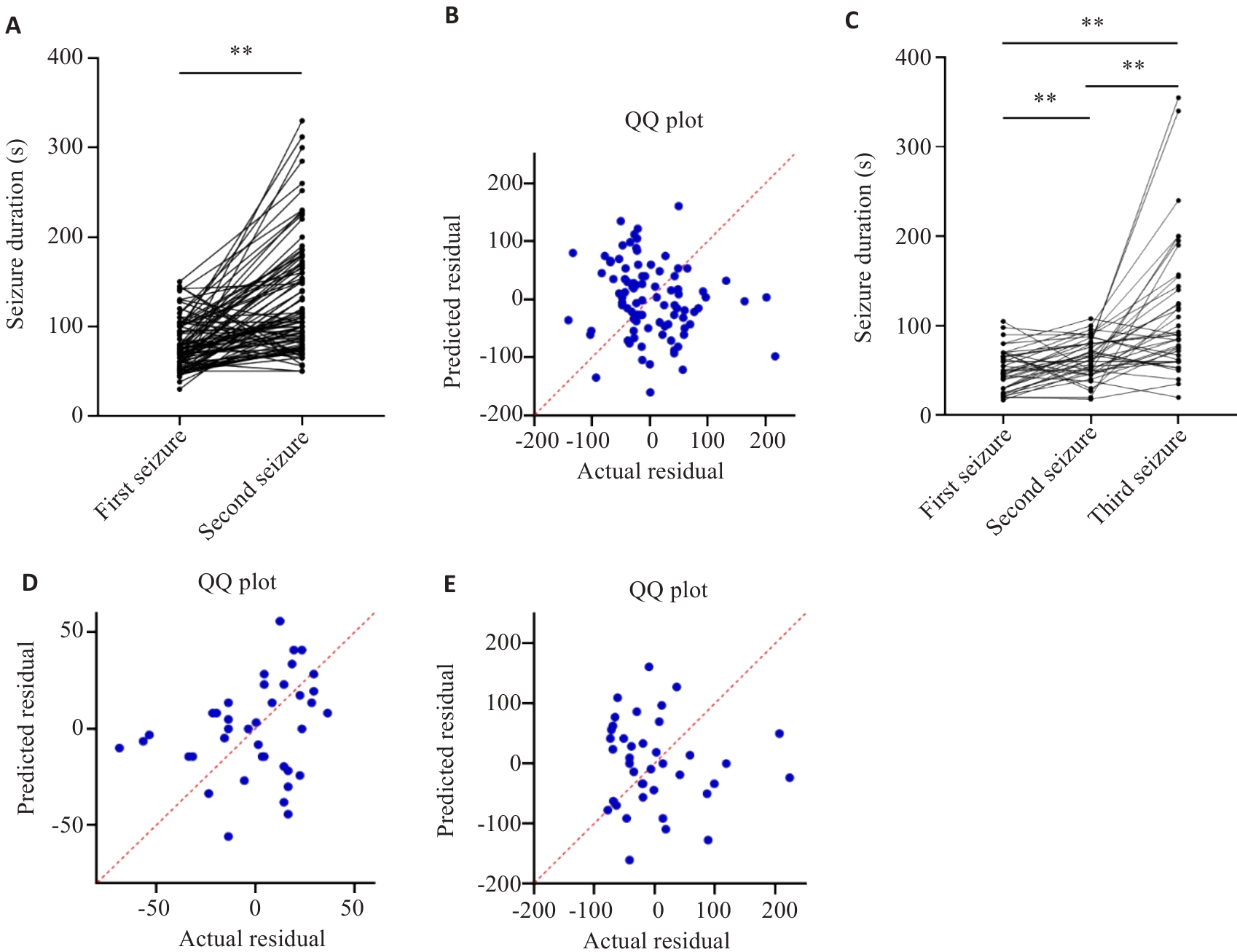
图3 EEG癫痫波发作时间分析
Fig.3 EEG seizure duration analysis. A, B: Correlation between the first and second seizure duration in E2 group. C-E: Correlation between the first, second and third seizure duration in E3 group. **P<0.01.
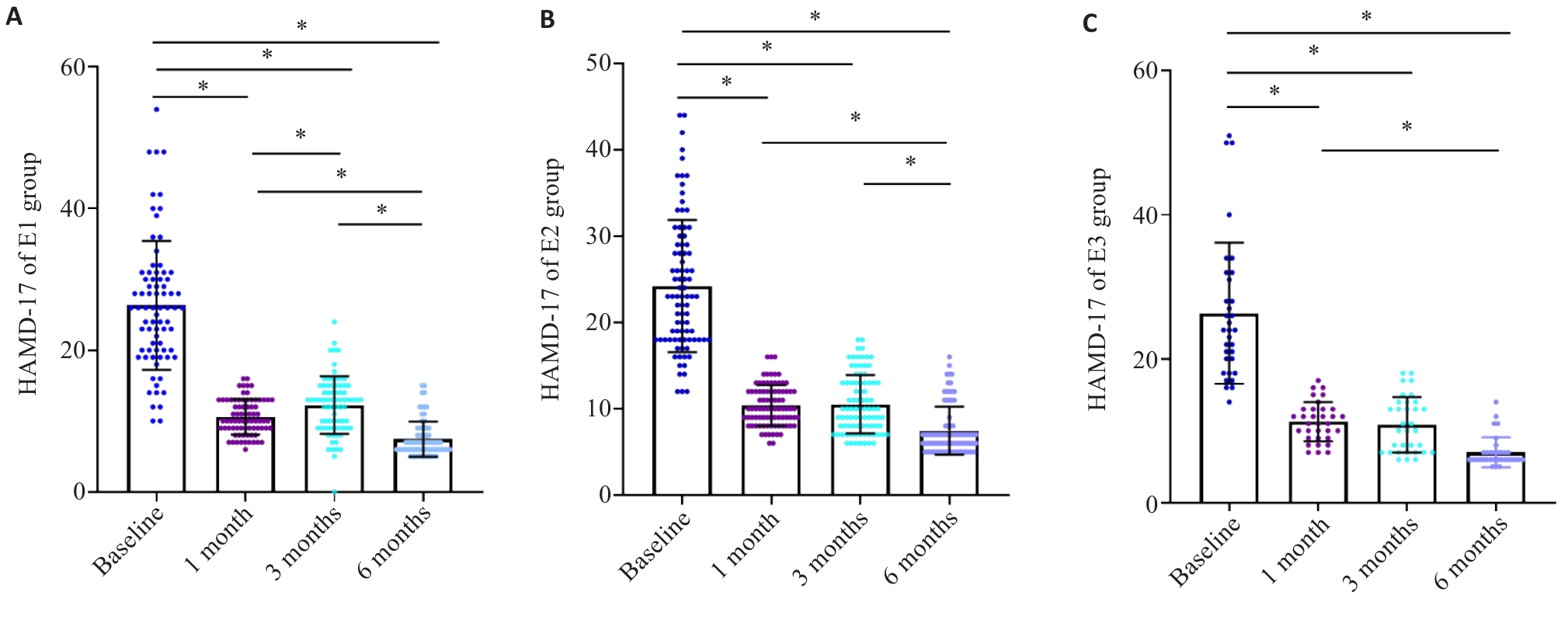
图4 基于HAMD-17评分的反应率分析
Fig.4 Response to super ECT assessed according to HAMD-17 scores relative to the baseline during the initial 6 months. A: HAMD-17 scores in E1 group. B: HAMD-17 scores in E2 group. C: HAMD-17 scores in E3 group. *P<0.05.
| Variables | E1 (n=88) | E2 (n=89) | E3 (n=39) | P |
|---|---|---|---|---|
Total response 1 month 3 months 6 months | 74 (84.09) 72 (81.82) 74 (84.09) | 84 (88.76) 81 (79.78) 76 (76.40) | 31 (79.48) 31 (79.48) 32 (82.05) | 0.634 0.863 0.790 |
Recovered 1 month 3 months 6 months | 5 (5.68) 5 (5,68) 30 (34.09) | 6 (6.74) 9 (10.11) 28 (31.46) | 2 (5.13) 4 (10.26) 10 (25.64) | 0.781 0.632 0.459 |
Significant improved 1 month 3 months 6 months | 56 (63.64) 40 (45.45) 42 (47.73) | 52 (58.43) 43 (48.31) 30 (33.71) | 23 (58.97) 18 (46.15) 20 (51.28) | 0.702 0.693 0.764 |
Improved 1 month 3 months 6 months | 13 (14.77) 27 (30.68) 2 (2.27) | 21 (23.59) 19 (21.35) 10 (11.24) | 6 (15.38) 9 (23.08) 2 (5.13) | 0.603 0.534 0.357 |
Ineffective 1 month 3 months 6 months | 2 (2.27) 4 (4.55) 2 (2.27) | 2 (2.25) 5 (5.62) 1 (1.12) | 2 (5.13) 2 (5.13) 1 (2.56) | 0.913 0.893 0.796 |
表3 首次治疗后1、3、6个月内基于HAMD-17减分率的疗效分析
Tab.3 Treatment response based on the reduction rate of HAMD-17 scores in 1 month, 3 months, and 6 months [n(%)]
| Variables | E1 (n=88) | E2 (n=89) | E3 (n=39) | P |
|---|---|---|---|---|
Total response 1 month 3 months 6 months | 74 (84.09) 72 (81.82) 74 (84.09) | 84 (88.76) 81 (79.78) 76 (76.40) | 31 (79.48) 31 (79.48) 32 (82.05) | 0.634 0.863 0.790 |
Recovered 1 month 3 months 6 months | 5 (5.68) 5 (5,68) 30 (34.09) | 6 (6.74) 9 (10.11) 28 (31.46) | 2 (5.13) 4 (10.26) 10 (25.64) | 0.781 0.632 0.459 |
Significant improved 1 month 3 months 6 months | 56 (63.64) 40 (45.45) 42 (47.73) | 52 (58.43) 43 (48.31) 30 (33.71) | 23 (58.97) 18 (46.15) 20 (51.28) | 0.702 0.693 0.764 |
Improved 1 month 3 months 6 months | 13 (14.77) 27 (30.68) 2 (2.27) | 21 (23.59) 19 (21.35) 10 (11.24) | 6 (15.38) 9 (23.08) 2 (5.13) | 0.603 0.534 0.357 |
Ineffective 1 month 3 months 6 months | 2 (2.27) 4 (4.55) 2 (2.27) | 2 (2.25) 5 (5.62) 1 (1.12) | 2 (5.13) 2 (5.13) 1 (2.56) | 0.913 0.893 0.796 |
| Variables | E1 (n=88) | E2 (n=89) | E3 (n=39) | P |
|---|---|---|---|---|
Side effects [n (%)] Fever Headache/dizziness General pain Dry mouth Nausea | 13 (14.77) 27 (30.68) 18 (20.45) 20 (22.73) 18 (20.45) | 21 (23.59) 28 (31.46) 9 (10.11) 17 (19.10) 19 (21.35) | 6 (15.38) 17 (43.58) 12 (30.76) 4 (10.26) 9 (23.08) | 0.764 0.213 0.179 0.452 0.812 |
Cognitive function assessment (Mean±SD) MMSE in pre-treatment MMSE in post-treatment | 27.13±1.24 27.3±3.79 | 26.83±2.03 26.76±2.99 | 27.41±2.15 26.85±3.73 | 0.559 0.794 |
表4 不良反应发生率和认知功能评估
Tab.4 Evaluation of the side effects of the treatment and cognitive function of the patients
| Variables | E1 (n=88) | E2 (n=89) | E3 (n=39) | P |
|---|---|---|---|---|
Side effects [n (%)] Fever Headache/dizziness General pain Dry mouth Nausea | 13 (14.77) 27 (30.68) 18 (20.45) 20 (22.73) 18 (20.45) | 21 (23.59) 28 (31.46) 9 (10.11) 17 (19.10) 19 (21.35) | 6 (15.38) 17 (43.58) 12 (30.76) 4 (10.26) 9 (23.08) | 0.764 0.213 0.179 0.452 0.812 |
Cognitive function assessment (Mean±SD) MMSE in pre-treatment MMSE in post-treatment | 27.13±1.24 27.3±3.79 | 26.83±2.03 26.76±2.99 | 27.41±2.15 26.85±3.73 | 0.559 0.794 |
| [1] | Friedrich MJ. Depression is the leading cause of disability around the world[J]. JAMA, 2017, 317(15): 1517. doi:10.1001/jama.2017.3826 |
| [2] | Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report[J]. Am J Psychiatry, 2006, 163(11): 1905-17. doi:10.1176/appi.ajp.163.11.1905 |
| [3] | Khin NA, Chen YF, Yang Y, et al. Exploratory analyses of efficacy data from major depressive disorder trials submitted to the US Food and Drug Administration in support of new drug applications[J]. J Clin Psychiatry, 2011, 72(4): 464-72. doi:10.4088/jcp.10m06191 |
| [4] | Kellner CH, Knapp RG, Petrides G, et al. Continuation electroconvulsive therapy vs pharmacotherapy for relapse prevention in major depression: a multisite study from the Consortium for Research in Electroconvulsive Therapy (CORE)[J]. Arch Gen Psychiatry, 2006, 63(12): 1337-44. doi:10.1001/archpsyc.63.12.1337 |
| [5] | Weiss A, Hussain S, Ng B, et al. Royal Australian and New Zealand College of Psychiatrists professional practice guidelines for the administration of electroconvulsive therapy[J]. Aust N Z J Psychiatry, 2019, 53(7): 609-23. doi:10.1177/0004867419839139 |
| [6] | Espinoza RT, Kellner CH. Electroconvulsive therapy[J]. N Engl J Med, 2022, 386(7): 667-72. doi:10.1056/nejmra2034954 |
| [7] | Liu CC, Qian XY, An JX, et al. Electroconvulsive therapy under general anesthesia with cisatracurium, laryngeal mask airways, and bispectral index[J]. J ECT, 2016, 32(1): 17-9. doi:10.1097/yct.0000000000000251 |
| [8] | McClintock SM, Choi J, Deng ZD, et al. Multifactorial determinants of the neurocognitive effects of electroconvulsive therapy[J]. J ECT, 2014, 30(2): 165-76. doi:10.1097/yct.0000000000000137 |
| [9] | van Duist M, Spaans HP, Verwijk E, et al. ECT non-remitters: prognosis and treatment after 12 unilateral electroconvulsive therapy sessions for major depression[J]. J Affect Disord, 2020, 272: 501-7. doi:10.1016/j.jad.2020.03.134 |
| [10] | Pennings CH, Van Boxtel M, De Korte-De Boer D, et al. Anaesthesia as a risk factor for long-term cognitive decline: Results of the prospective MAAS cohort study[J]. Eur J Anaesthesiol, 2025, 42(5): 468-77. doi:10.1097/eja.0000000000002133 |
| [11] | Dandekar MP, Diaz AP, Rahman Z, et al. A narrative review on invasive brain stimulation for treatment-resistant depression[J]. Braz J Psychiatry, 2022, 44(3): 317-30. doi:10.1590/1516-4446-2021-1874 |
| [12] | Bewernick B, Schlaepfer TE. Update on neuromodulation for treatment-resistant depression[J]. F1000Research, 2015, 4: 1389. doi:10.12688/f1000research.6633.1 |
| [13] | Peterchev AV, Rosa MA, Deng ZD, et al. Electroconvulsive therapy stimulus parameters: rethinking dosage[J]. J ECT, 2010, 26(3): 159-74. doi:10.1097/yct.0b013e3181e48165 |
| [14] | Bakewell CJ, Russo J, Tanner C, et al. Comparison of clinical efficacy and side effects for bitemporal and bifrontal electrode placement in electroconvulsive therapy[J]. J ECT, 2004, 20(3): 145-53. doi:10.1097/00124509-200409000-00005 |
| [15] | Tor PC, Bautovich A, Wang MJ, et al. A systematic review and meta-analysis of brief versus ultrabrief right unilateral electroconvulsive therapy for depression[J]. J Clin Psychiatry, 2015, 76(9): e1092-8. doi:10.4088/jcp.14r09145 |
| [16] | Luccarelli J, McCoy TH Jr, Seiner SJ, et al. Changes in seizure duration during acute course electroconvulsive therapy[J]. Brain Stimul, 2021, 14(4): 941-6. doi:10.1016/j.brs.2021.05.016 |
| [17] | McCabe GA, Smith MM, Widiger TA. Psychopathy and antisocial personality disorder in the fifth edition of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders: an attempted replication of Wygantet al. (2016)[J]. Pers Disord Theory Res Treat, 2023, 14(6): 636-48. doi:10.1037/per0000626 |
| [18] | Han CS, Wang G, Chan S, et al. Definition and identification of patients with treatment-resistant depression in real-world clinical practice settings across Asia[J]. Neuropsychiatr Dis Treat, 2020, 16: 2929-41. doi:10.2147/ndt.s264799 |
| [19] | Kronsell A, Nordenskjöld A, Bell M, et al. The effect of anaesthetic dose on response and remission in electroconvulsive therapy for major depressive disorder: nationwide register-based cohort study[J]. BJPsych Open, 2021, 7(2): e71. doi:10.1192/bjo.2021.31 |
| [20] | Weinger MB, Partridge BL, Hauger R, et al. Prevention of the cardiovascular and neuroendocrine response to electroconvulsive therapy: I. Effectiveness of pretreatment regimens on hemodynamics[J]. Anesth Analg, 1991, 73(5): 556-62. doi:10.1213/00000539-199111000-00008 |
| [21] | Maixner DF, Weiner R, Reti IM, et al. Electroconvulsive therapy is an essential procedure[J]. Am J Psychiatry, 2021, 178(5): 381-2. doi:10.1176/appi.ajp.2020.20111647 |
| [22] | Pluijms EM, Birkenhäger TK, Huijbrechts IPAM, et al. Influence of resistance to antidepressant pharmacotherapy on short-term response to electroconvulsive therapy[J]. J Affect Disord, 2002, 69(1/2/3): 93-9. doi:10.1016/s0165-0327(00)00378-5 |
| [23] | Kho KH, Zwinderman AH, Blansjaar BA. Predictors for the efficacy of electroconvulsive therapy: chart review of a naturalistic study[J]. J Clin Psychiatry, 2005, 66(7): 894-9. doi:10.4088/jcp.v66n0712 |
| [24] | Goldfarb S, Fainstein N, Ganz T, et al. Electric neurostimulation regulates microglial activation via retinoic acid receptor α signaling[J]. Brain Behav Immun, 2021, 96: 40-53. doi:10.1016/j.bbi.2021.05.007 |
| [25] | Sackeim HA, Haskett RF, Mulsant BH, et al. Continuation pharmacotherapy in the prevention of relapse following electroconvulsive therapy: a randomized controlled trial[J]. JAMA, 2001, 285(10): 1299-307. doi:10.1001/jama.285.10.1299 |
| [26] | Fink M. What is an adequate treatment in convulsive therapy?[J]. Acta Psychiatr Scand, 1991, 84(5): 424-7. doi:10.1111/j.1600-0447.1991.tb03172.x |
| [27] | Brus O, Cao Y, Gustafsson E, et al. Self-assessed remission rates after electroconvulsive therapy of depressive disorders[J]. Eur Psychiatry, 2017, 45: 154-60. doi:10.1016/j.eurpsy.2017.06.015 |
| [28] | Haas S, Nash K, Lippmann SB. ECT-induced seizure durations[J]. J Ky Med Assoc, 1996, 94(6): 233-6. |
| [29] | Kales H, Raz J, Tandon R, et al. Relationship of seizure duration to antidepressant efficacy in electroconvulsive therapy[J]. Psychol Med, 1997, 27(6): 1373-80. doi:10.1017/s0033291797005564 |
| [30] | Nishikawa K, Yamakage M. Effects of the concurrent use of a reduced dose of propofol with divided supplemental remifentanil and moderate hyperventilation on duration and morphology of electroconvulsive therapy-induced electroencephalographic seizure activity: a randomized controlled trial[J]. J Clin Anesth, 2017, 37: 63-8. doi:10.1016/j.jclinane.2016.11.006 |
| [31] | O’Connor MK, Knapp R, Husain M, et al. The influence of age on the response of major depression to electroconvulsive therapy: a C.O.R.E. Report[J]. Am J Geriatr Psychiatry, 2001, 9(4): 382-90. doi:10.1176/appi.ajgp.9.4.382 |
| [32] | Zolezzi M. Medication management during electroconvulsant therapy[J]. Neuropsychiatr Dis Treat, 2016, 12: 931-9. doi:10.2147/ndt.s100908 |
| [33] | Radman T, Lisanby SH. New directions in the rational design of electrical and magnetic seizure therapies: individualized Low Amplitude Seizure Therapy (iLAST) and Magnetic Seizure Therapy (MST)[J]. Int Rev Psychiatry, 2017, 29(2): 63-78. doi:10.1080/09540261.2017.1304898 |
| [34] | Phutane VH, Thirthalli J, Muralidharan K, et al. Double-blind randomized controlled study showing symptomatic and cognitive superiority of bifrontal over bitemporal electrode placement during electroconvulsive therapy for schizophrenia[J]. Brain Stimul, 2013, 6(2): 210-7. doi:10.1016/j.brs.2012.04.002 |
| [35] | Hu YD, Xiang YT, Fang JX, et al. Single i.v. ketamine augmentation of newly initiated escitalopram for major depression: results from a randomized, placebo-controlled 4-week study[J]. Psychol Med, 2016, 46(3): 623-35. doi:10.1017/s0033291715002159 |
| [36] | Phillips JL, Norris S, Talbot J, et al. Single, repeated, and maintenance ketamine infusions for treatment-resistant depression: a randomized controlled trial[J]. Am J Psychiatry, 2019, 176(5): 401-9. doi:10.1176/appi.ajp.2018.18070834 |
| [37] | Erdil F, Ozgul U, Çolak C, et al. Effect of the addition of ketamine to sevoflurane anesthesia on seizure duration in electroconvulsive therapy[J]. J ECT, 2015, 31(3): 182-5. doi:10.1097/yct.0000000000000225 |
| [38] | Kranaster L, Kammerer-Ciernioch J, Hoyer C, et al. Clinically favourable effects of ketamine as an anaesthetic for electroconvulsive therapy: a retrospective study[J]. Eur Arch Psychiatry Clin Neurosci, 2011, 261(8): 575-82. doi:10.1007/s00406-011-0205-7 |
| [39] | Menon V, Varadharajan N, Faheem A, et al. Ketamine vs electroconvulsive therapy for major depressive episode: a systematic review and meta-analysis[J]. JAMA Psychiatry, 2023, 80(6): 639-42. doi:10.1001/jamapsychiatry.2023.0562 |
| [40] | Rhee TG, Shim SR, Forester BP, et al. Efficacy and safety of ketamine vs electroconvulsive therapy among patients with major depressive episode: a systematic review and meta-analysis[J]. JAMA Psychiatry, 2022, 79(12): 1162-72. doi:10.1001/jamapsychiatry.2022.3352 |
| [41] | Read J, Harrop C, Geekie J. Time to acknowledge the bias of some electroconvulsive therapy researchers and defenders[J]. Lancet Psychiatry, 2022, 9(2): e9. doi:10.1016/s2215-0366(21)00506-x |
| No related articles found! |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||