南方医科大学学报 ›› 2024, Vol. 44 ›› Issue (7): 1407-1415.doi: 10.12122/j.issn.1673-4254.2024.07.21
• • 上一篇
潘甚豪1,2( ), 李炎坤1,2, 伍哲维1,2, 毛玉玲1, 王春艳1()
), 李炎坤1,2, 伍哲维1,2, 毛玉玲1, 王春艳1()
收稿日期:2024-05-15
出版日期:2024-07-20
发布日期:2024-07-25
通讯作者:
王春艳
E-mail:psh@stu.gzhmu.edu.cn;wangchunyan@zju.edu.cn
作者简介:潘甚豪,在读本科生,E-mail: psh@stu.gzhmu.edu.cn
基金资助:
Shenhao PAN1,2(), Yankun LI1,2, Zhewei WU1,2, Yuling MAO1, Chunyan WANG1()
Received:2024-05-15
Online:2024-07-20
Published:2024-07-25
Contact:
Chunyan WANG
E-mail:psh@stu.gzhmu.edu.cn;wangchunyan@zju.edu.cn
Supported by:摘要:
目的 构建并验证子宫内膜异位症(EMs)患者辅助生殖治疗(ART)中新鲜胚胎移植的临床妊娠率预测模型。 方法 选取2017年5月~2023年11月在本院生殖医学中心进行ART治疗的464例子宫内膜异位症不孕患者,并将其分为建模人群(60%)和验证人群(40%)。采用单因素分析、多因素Logistic回归分析、LASSO回归分析EMs患者新鲜胚胎移植妊娠率的相关因素,并建立预测EMs患者新鲜胚胎移植临床妊娠率的列线图模型。采用ROC的曲线下面积(AUC)、校准曲线和决策曲线分别在建模人群和验证人群对预测模型进行验证。为提高模型性能,本研究采用Stacking集成学习方法集成GBM、XGBOOST、MLP 3种机器学习方法,利用它们各自优势相互补充以提高模型预测性能。 结果 女性年龄、Gn启动用量、ART次数、移植胚胎数是影响新鲜胚胎移植临床妊娠率的独立因素(P<0.05)。通过LASSO模型筛选纳入变量:女性年龄、FSH、Gn时间、Gn启动用量、ART次数、获卵数、移植胚胎数、HCG日内膜厚度、HCG日P。训练集中,模型准确性为0.642(95% CI:0.605-0.679),测试集中,模型准确性为0.652(95% CI:0.600-0.704)。集成学习方法可以提高模型的性能:训练集中,模型准确性为0.725(95% CI:0.680-0.770),测试集中,模型准确性为0.718(95% CI:0.675-0.761)。 结论 本研究所建立预测模型有助于预测子宫内膜异位症患者新鲜胚胎移植的临床妊娠率,为子宫内膜异位症ART治疗提供指导意见。
潘甚豪, 李炎坤, 伍哲维, 毛玉玲, 王春艳. 子宫内膜异位症患者新鲜胚胎移植临床妊娠率预测模型的建立与验证[J]. 南方医科大学学报, 2024, 44(7): 1407-1415.
Shenhao PAN, Yankun LI, Zhewei WU, Yuling MAO, Chunyan WANG. Establishment of a predictive nomogram for clinical pregnancy rate in patients with endometriosis undergoing fresh embryo transfer[J]. Journal of Southern Medical University, 2024, 44(7): 1407-1415.
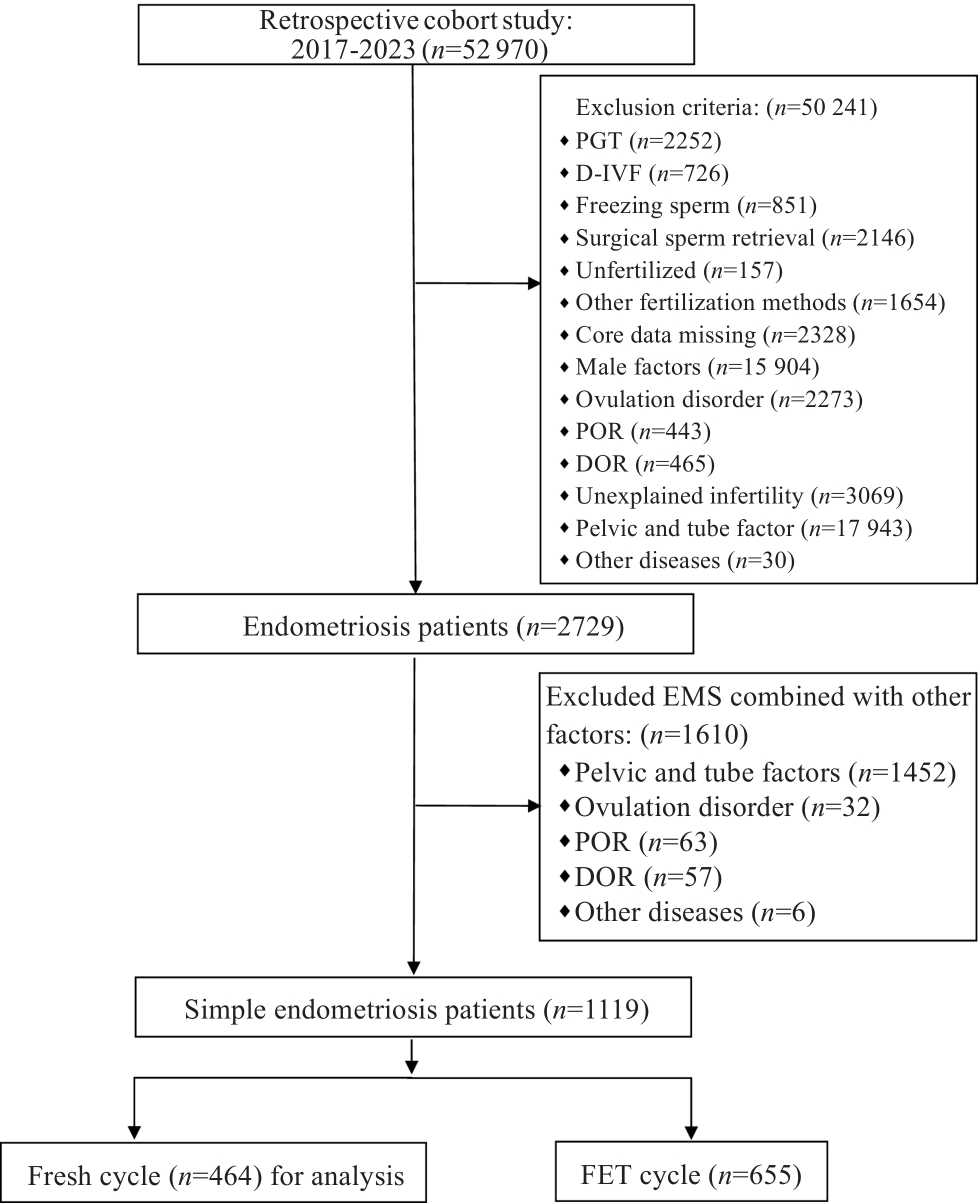
图1 研究对象筛选流程图
Fig 1 Flowchart of subject selection. Sample size (n) is indicated in each category. PGT: Preimplantation genetic testing; D-IVF: Sperm donation-in vitro fertilization; DOR: Diminished ovarian reserve; POR: Poor ovarian response; FET: Frozen embryo transfer.
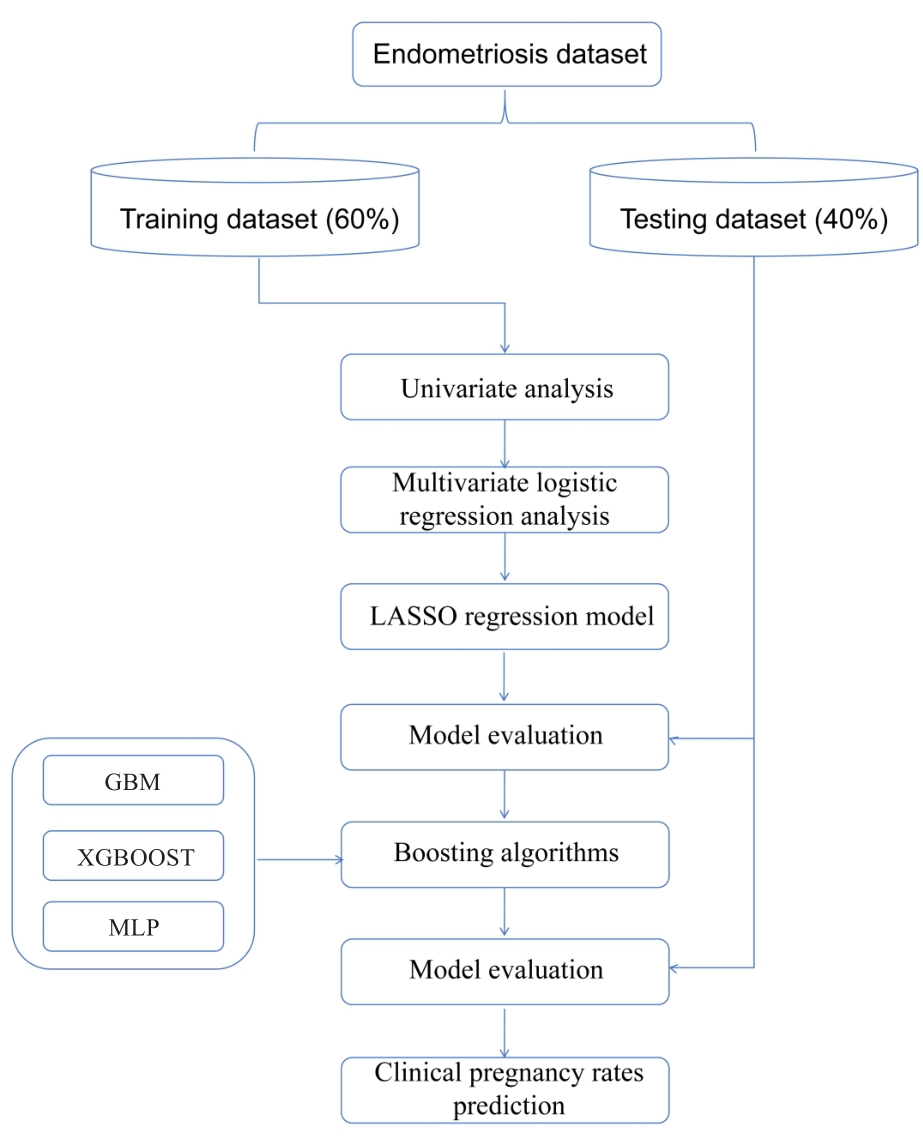
图2 研究工作的分析方法
Fig.2 Proposed methodology for research work. LightGBM: Light gradient boosting machine; XGBoost: Extreme Gradient Boosting; MLP: Multi-Layer Perceptron.
| Variables | Pregnancy (n=254) | Unpregnancy (n=210) | t/χ² | P |
|---|---|---|---|---|
| Age (year) | 32.19±3.58 | 33.70±4.43 | -4.008 | <0.001 |
| BMI(kg/m2) | 21.22±3.00 | 21.66±2.87 | -1.596 | 0.111 |
| AMH (ng/mL) | 3.19±2.23 | 2.81±2.10 | 1.872 | 0.062 |
| Infertility time in years | 4.00±2.55 | 4.35±2.81 | -1.358 | 0.175 |
| Type of subfertility | 0.345 | 0.571 | ||
| Primary infertility | 102 | 90 | ||
| Secondary infertility | 152 | 120 | ||
| FSH (U/L) | 5.92±2.44 | 6.54±3.06 | -2.447 | 0.015 |
| LH (U/L) | 4.35±5.80 | 3.70±2.93 | 1.554 | 0.121 |
| P (nmol/L) | 1.69±6.80 | 1.61±5.55 | 0.137 | 0.891 |
| PRL (ng/mL) | 17.24±8.85 | 16.31±8.87 | 1.124 | 0.262 |
| T (nmol/L) | 0.98±0.46 | 1.00±0.41 | -0.611 | 0.541 |
| E2 (pg/mL) | 220.95±365.46 | 179.90±196.84 | 1.540 | 0.124 |
| Dates of Gn Duration | 11.14±2.28 | 10.78±2.38 | 1.650 | 0.100 |
| Total Gn (IU) | 2356.74±1166.58 | 2423.30±1018.86 | -0.652 | 0.515 |
| Gn initation dose | 190.25±60.69 | 211.22±67.40 | -3.526 | <0.001 |
| E2 on HCG day (pg/mL) | 8062.67±3937.74 | 7527.33±4201.39 | 1.414 | 0.158 |
| P on HCG day (nmol/L) | 2.04±0.94 | 2.20±1.01 | -1.714 | 0.087 |
| Follicles≥14 mm on HCG day | 6.45±4.32 | 5.80±4.19 | 1.633 | 0.103 |
| Endometrium thickness on HCG day (mm) | 11.46±2.22 | 11.10±2.42 | 1.665 | 0.097 |
| Oocytes retrieved | 9.09±3.92 | 8.19±4.31 | 2.366 | 0.018 |
| ART Cycles | 1.33±0.68 | 1.55±1.07 | -2.607 | 0.010 |
| Fertilization rate (%) | 83.58±17.52 | 81.50±20.29 | 1.174 | 0.241 |
| Normal Fertilization rate (%) | 59.92±23.11 | 60.99±23.67 | -0.492 | 0.623 |
| degeneration rate(%) | 2.97±8.24 | 3.24±1.43 | -0.252 | 0.801 |
| Cleavage rate (%) | 98.59±5.00 | 97.45±10.38 | 1.495 | 0.136 |
| Usable embryos rate (%) | 56.53±26.37 | 53.74±26.88 | 1.127 | 0.260 |
| High quality day 3 embyo (%) | 28.43±26.93 | 24.61±30.07 | 1.442 | 0.150 |
| Blastulation rate (%) | 33.08±33.81 | 31.50±33.41 | 0.506 | 0.613 |
| Number of frozen embryos | 2.08±2.05 | 1.58±1.91 | 2.716 | 0.007 |
| Embryo transfer (n) | 1.65±0.48 | 1.48±0.50 | 3.700 | <0.001 |
表1 临床妊娠率与患者基本特征、周期信息、实验室结局单因素分析
Tab.1 Univariate analysis of factors affecting clinical pregnancy
| Variables | Pregnancy (n=254) | Unpregnancy (n=210) | t/χ² | P |
|---|---|---|---|---|
| Age (year) | 32.19±3.58 | 33.70±4.43 | -4.008 | <0.001 |
| BMI(kg/m2) | 21.22±3.00 | 21.66±2.87 | -1.596 | 0.111 |
| AMH (ng/mL) | 3.19±2.23 | 2.81±2.10 | 1.872 | 0.062 |
| Infertility time in years | 4.00±2.55 | 4.35±2.81 | -1.358 | 0.175 |
| Type of subfertility | 0.345 | 0.571 | ||
| Primary infertility | 102 | 90 | ||
| Secondary infertility | 152 | 120 | ||
| FSH (U/L) | 5.92±2.44 | 6.54±3.06 | -2.447 | 0.015 |
| LH (U/L) | 4.35±5.80 | 3.70±2.93 | 1.554 | 0.121 |
| P (nmol/L) | 1.69±6.80 | 1.61±5.55 | 0.137 | 0.891 |
| PRL (ng/mL) | 17.24±8.85 | 16.31±8.87 | 1.124 | 0.262 |
| T (nmol/L) | 0.98±0.46 | 1.00±0.41 | -0.611 | 0.541 |
| E2 (pg/mL) | 220.95±365.46 | 179.90±196.84 | 1.540 | 0.124 |
| Dates of Gn Duration | 11.14±2.28 | 10.78±2.38 | 1.650 | 0.100 |
| Total Gn (IU) | 2356.74±1166.58 | 2423.30±1018.86 | -0.652 | 0.515 |
| Gn initation dose | 190.25±60.69 | 211.22±67.40 | -3.526 | <0.001 |
| E2 on HCG day (pg/mL) | 8062.67±3937.74 | 7527.33±4201.39 | 1.414 | 0.158 |
| P on HCG day (nmol/L) | 2.04±0.94 | 2.20±1.01 | -1.714 | 0.087 |
| Follicles≥14 mm on HCG day | 6.45±4.32 | 5.80±4.19 | 1.633 | 0.103 |
| Endometrium thickness on HCG day (mm) | 11.46±2.22 | 11.10±2.42 | 1.665 | 0.097 |
| Oocytes retrieved | 9.09±3.92 | 8.19±4.31 | 2.366 | 0.018 |
| ART Cycles | 1.33±0.68 | 1.55±1.07 | -2.607 | 0.010 |
| Fertilization rate (%) | 83.58±17.52 | 81.50±20.29 | 1.174 | 0.241 |
| Normal Fertilization rate (%) | 59.92±23.11 | 60.99±23.67 | -0.492 | 0.623 |
| degeneration rate(%) | 2.97±8.24 | 3.24±1.43 | -0.252 | 0.801 |
| Cleavage rate (%) | 98.59±5.00 | 97.45±10.38 | 1.495 | 0.136 |
| Usable embryos rate (%) | 56.53±26.37 | 53.74±26.88 | 1.127 | 0.260 |
| High quality day 3 embyo (%) | 28.43±26.93 | 24.61±30.07 | 1.442 | 0.150 |
| Blastulation rate (%) | 33.08±33.81 | 31.50±33.41 | 0.506 | 0.613 |
| Number of frozen embryos | 2.08±2.05 | 1.58±1.91 | 2.716 | 0.007 |
| Embryo transfer (n) | 1.65±0.48 | 1.48±0.50 | 3.700 | <0.001 |
| Variables | B | χ² | P | OR | 95% CI |
|---|---|---|---|---|---|
| Age (year) | -0.075 | 7.990 | 0.005 | 0.928 | 0.881-0.977 |
| Gn initation dose | -0.003 | 4.495 | 0.034 | 0.997 | 0.993-1.000 |
| ART Cycles | -0.247 | 4.207 | 0.040 | 0.781 | 0.617-0.989 |
| Embryo transfer (n) | 0.838 | 17.492 | <0.001 | 2.311 | 1.561-3.422 |
表2 多因素Logistic回归分析
Tab.2 Multivariate logistic regression analysis of key clinical features affecting pregnancy outcomes
| Variables | B | χ² | P | OR | 95% CI |
|---|---|---|---|---|---|
| Age (year) | -0.075 | 7.990 | 0.005 | 0.928 | 0.881-0.977 |
| Gn initation dose | -0.003 | 4.495 | 0.034 | 0.997 | 0.993-1.000 |
| ART Cycles | -0.247 | 4.207 | 0.040 | 0.781 | 0.617-0.989 |
| Embryo transfer (n) | 0.838 | 17.492 | <0.001 | 2.311 | 1.561-3.422 |
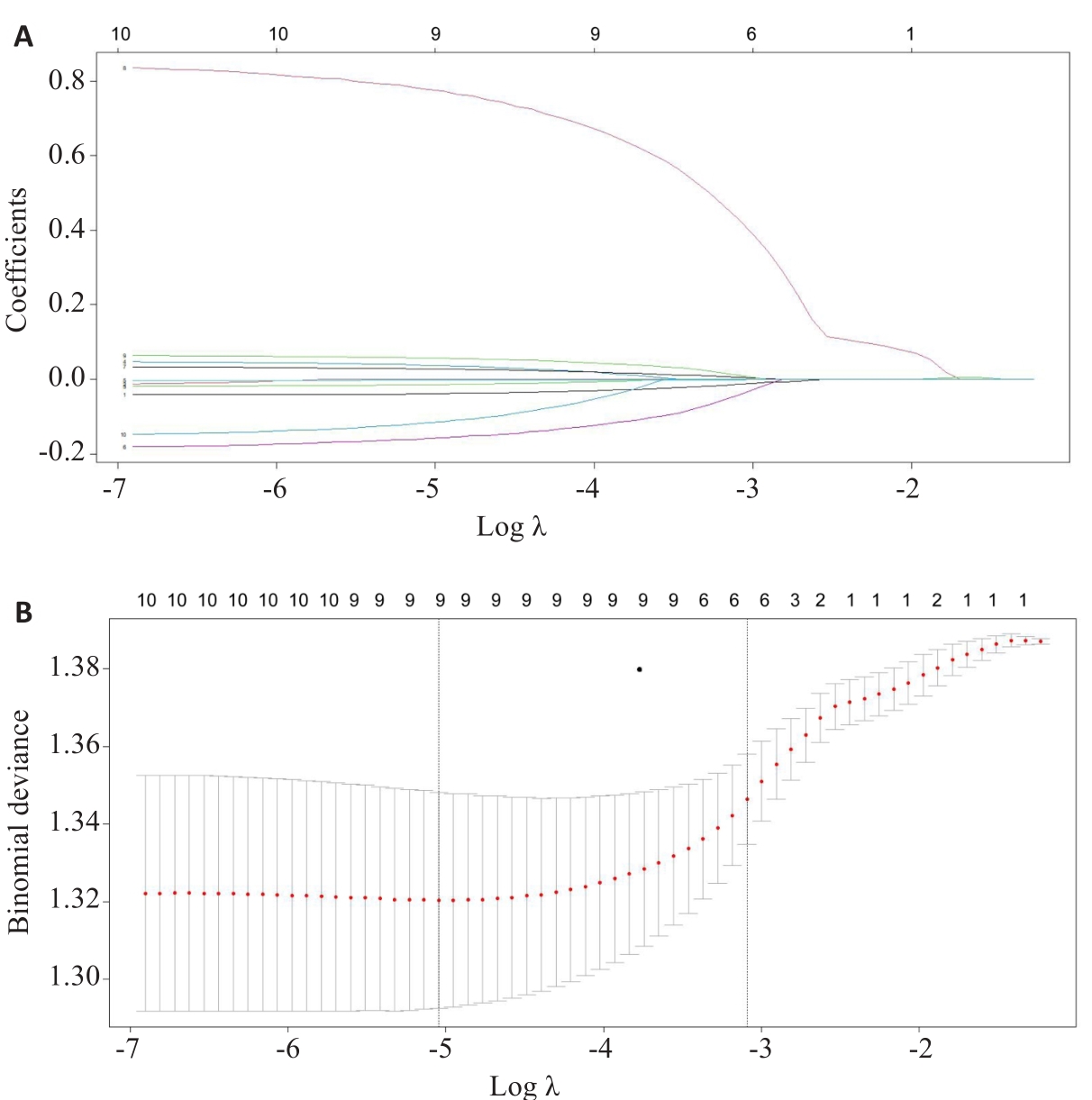
图3 LASSO 回归分析
Fig.3 LASSO regression model. A: Coefficient distribution chart by lasso regression. Each curve represents a coefficient, and the x-axis represents the regularization penalty parameter. As λ changes, a coefficient that becomes non-zero enters the LASSO regression model. B: Ten-fold cross-validation diagram. The red dotted vertical line crosses over the optimal log λ. The two dotted lines represent one standard deviation from the minimum value, with 1se as the criterion (λ=0.006438551).
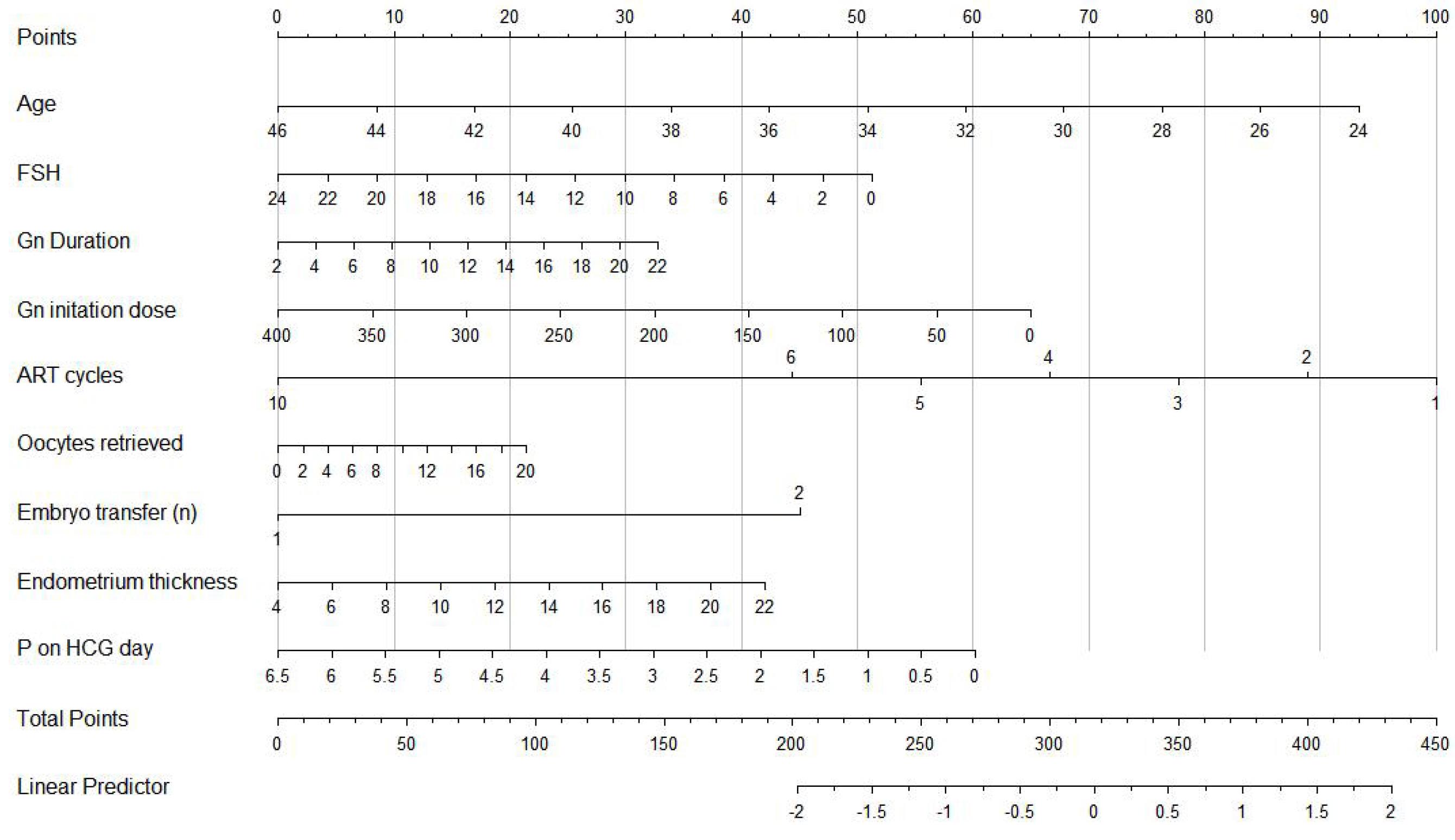
图4 子宫内膜异位症患者新鲜胚胎移植临床妊娠率的Nomogram预测模型
Fig.4 Nomogram of the prediction model for clinical pregnancy in endometriosis patients undergoing fresh embryo transfer. The nomogram is applied by drawing a perpendicular line from each risk factor's corresponding axis to intersect with the "Points" top line, followed by calculation of the total score as the sum of points for all risk factors, drawing a descending line from the "Total points" axis to intercept with the lower line, and determination of the probability of clinical pregnancy.
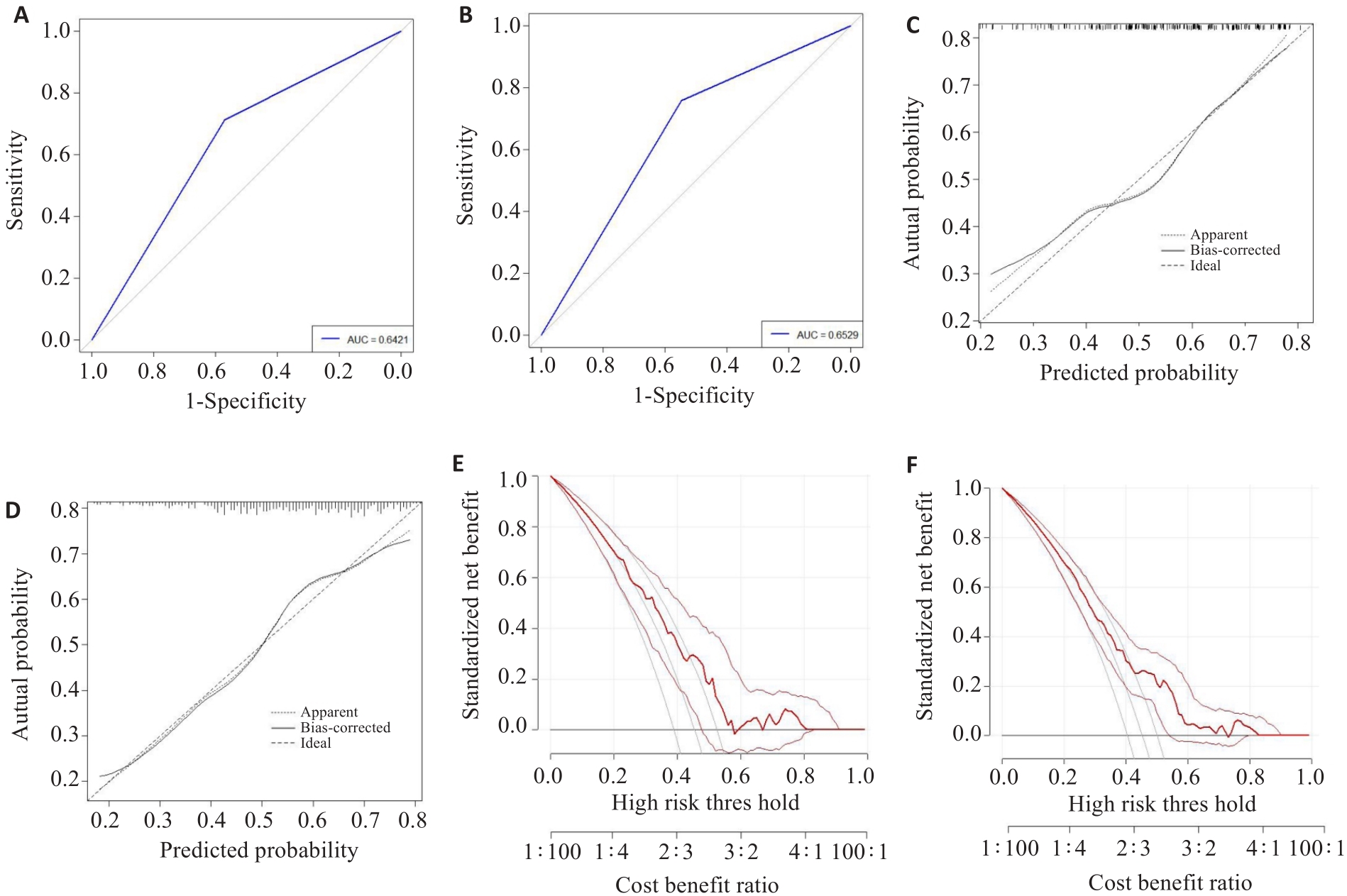
图5 列线图预测模型的验证及临床实用性
Fig.5 Validation of accuracy and discrimination of the nomogram model. A, B: ROC for training and validation cohorts. C, D: Calibration curves for evaluating calibration of the model: The horizontal axis is the predicted probability provided by this model, and the vertical axis is the observed incidence of pregnancy failure. The ideal line with 45° slope represents a perfect prediction (the predicted probability equals the observed probability; E, F: Decision curve of the prediction model.
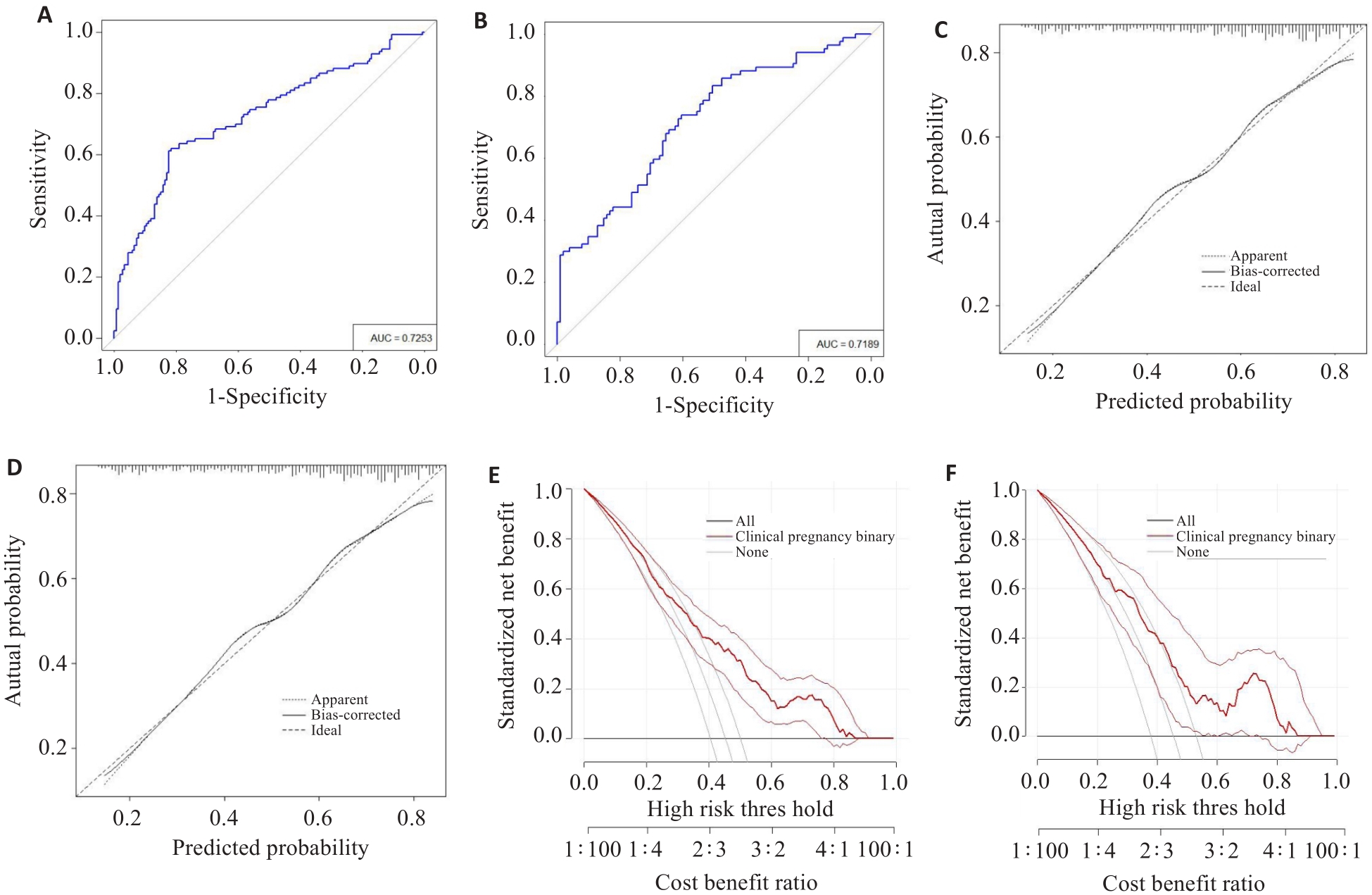
图6 集成学习提高预测模型的性能
Fig.6 Ensemble learning improves the performance of the predictive models. A, B: ROC for training and validation cohorts; C, D: Calibration curves for evaluating calibration of the training and validation cohorts. E, F: Decision curve of the training and validation cohorts.
| 1 | Saunders PTK, Horne AW. Endometriosis: Etiology, pathobiology, and therapeutic prospects[J]. Cell, 2021, 184(11): 2807-24. |
| 2 | Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations[J]. Lancet, 2021, 397(10276): 839-52. |
| 3 | Simoens S, Dunselman G, Dirksen C, et al. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres[J]. Hum Reprod, 2012, 27(5): 1292-9. |
| 4 | Ata B, Somigliana E. Endometriosis, staging, infertility and assisted reproductive technology: time for a rethink[J]. Reprod Biomed Online, 2024, 49(1): 103943. |
| 5 | Pais AS, Almeida-Santos T. Recent insights explaining susceptibility to endometriosis-From genetics to environment[J]. WIREs Mech Dis, 2023, 15(6): e1624. |
| 6 | Huang Y, Wang Z, Li B, et al. Loss of KLF15 impairs endometrial receptivity by inhibiting EMT in endometriosis[J]. J Endocrinol, 2024, 261(2): e230319. |
| 7 | Melado L, Ata B. Chapter 11. Endometriosis-related complications in women undergoing in-vitro fertilization[J]. Best Pract Res Clin Obstet Gynaecol, 2024, 93: 102456. |
| 8 | Bourdon M, Peigné M, Maignien C, et al. Impact of endometriosis surgery on in vitro fertilization/intracytoplasmic sperm injection outcomes: a systematic review and meta-analysis[J]. Reprod Sci, 2024, 31(6): 1431-55. |
| 9 | Ozer G, Akca A, Yuksel B, et al. Prediction of risk factors for first trimester pregnancy loss in frozen-thawed good-quality embryo transfer cycles using machine learning algorithms[J]. J Assist Reprod Genet, 2023, 40(2): 279-88. |
| 10 | Gao H, Liu DE, Li YM, et al. Early prediction of live birth for assisted reproductive technology patients: a convenient and practical prediction model[J]. Sci Rep, 2021, 11: 331. |
| 11 | Huang FP, Zhang HL, Xie X, et al. A model for pregnancy rates after IVF-ET in patients with infertility and endometriosis[J]. Eur Rev Med Pharmacol Sci, 2022, 26(19): 7188-94. |
| 12 | Ballester M, Oppenheimer A, Mathieu d' Argent E, et al. Nomogram to predict pregnancy rate after ICSI-IVF cycle in patients with endometriosis[J]. Hum Reprod, 2012, 27(2): 451-6. |
| 13 | Kordus RJ, LaVoie HA. Granulosa cell biomarkers to predict pregnancy in ART: pieces to solve the puzzle[J]. Reproduction, 2017, 153(2): R69-83. |
| 14 | Jin H, Shen X, Song W, et al. The development of nomograms to predict blastulation rate following cycles of in vitro fertilization in patients with tubal factor infertility, polycystic ovary syndrome, or endometriosis[J]. Front Endocrinol: Lausanne, 2021, 12: 751373. |
| 15 | Zhu S, Liao X, Jiang W, et al. Development and validation of a nomogram model for predicting clinical pregnancy in endometriosis patients undergoing fresh embryo transfer[J]. BMC Pregnancy Childbirth, 2023, 23(1): 764. |
| 16 | Riley RD, Ensor J, Snell KIE, et al. Calculating the sample size required for developing a clinical prediction model[J]. BMJ, 2020: m441. |
| 17 | Diakiw SM, Hall JMM, VerMilyea MD, et al. Development of an artificial intelligence model for predicting the likelihood of human embryo euploidy based on blastocyst images from multiple imaging systems during IVF[J]. Hum Reprod, 2022, 37(8): 1746-59. |
| 18 | Majumdar G, Majumdar A, Verma IC, et al. Relationship between morphology, euploidy and implantation potential of cleavage and blastocyst stage embryos[J]. J Hum Reprod Sci, 2017, 10(1): 49-57. |
| 19 | Lin XN, Wei ML, Tong XM, et al. Outcome of in vitro fertilization in endometriosis-associated infertility: a 5-year database cohort study[J]. Chin Med J: Engl, 2012, 125(15): 2688-93. |
| 20 | de Ziegler D, Pirtea P, Carbonnel M, et al. Assisted reproduction in endometriosis[J]. Best Pract Res Clin Endocrinol Metab, 2019, 33(1): 47-59. |
| 21 | Härkki P, Tiitinen A, Ylikorkala O. Endometriosis and assisted reproduction techniques[J]. Ann N Y Acad Sci, 2010, 1205: 207-13. |
| 22 | Osmanlıoğlu Ş, Berker B, Aslan B, et al. Presence of endometrioma does not impair embryo quality and assisted reproductive technology (ART) cycle outcome in diminished ovarian reserve (DOR) patients[J]. Reprod Sci, 2023, 30(5): 1540-7. |
| 23 | Barbosa MA, Teixeira DM, Navarro PA, et al. Impact of endometriosis and its staging on assisted reproduction outcome: systematic review and meta-analysis[J]. Ultrasound Obstet Gynecol, 2014, 44(3): 261-78. |
| 24 | Bourdon M, Dahan Y, Maignien C, et al. Influence of endometrioma size on ART outcomes[J]. Reprod Biomed Online, 2022, 45(6): 1237-46. |
| 25 | Wang XZ, Li WS, Chen XM, et al. Is the long-acting gonadotropin-releasing hormone agonist longprotocol better for patients with endometriosis undergoing IVF[J]? Int J Gynecol Obstet, 2023, 162(1): 325-32. |
| 26 | Hernández A, Sanz A, Spagnolo E, et al. Impact of ovarian endometrioma and surgery on reproductive outcomes: a single-center Spanish cohort study[J]. Biomedicines, 2023, 11(3): 844. |
| 27 | Hong IS. Endometrial stem/progenitor cells: properties, origins, and functions[J]. Genes Dis, 2023, 10(3): 931-47. |
| 28 | Labarta E, Martínez-Conejero JA, Alamá P, et al. Endometrial receptivity is affected in women with high circulating progesterone levels at the end of the follicular phase: a functional genomics analysis[J]. Hum Reprod, 2011, 26(7): 1813-25. |
| 29 | Ganie SM, Pramanik PKD, Bashir Malik M, et al. An ensemble learning approach for diabetes prediction using boosting techniques[J]. Front Genet, 2023, 14: 1252159. |
| [1] | 申采玉, 王帅, 周锐盈, 汪雨贺, 高琴, 陈兴智, 杨枢. 慢性心力衰竭合并肺部感染患者院内死亡风险预测:基于可解释性机器学习方法[J]. 南方医科大学学报, 2024, 44(6): 1141-1148. |
| [2] | 戈 悦, 李建伟, 梁宏开, 侯六生, 左六二, 陈 珍, 卢剑海, 赵 新, 梁静漪, 彭 岚, 包静娜, 段佳欣, 刘 俐, 毛可晴, 曾振华, 胡鸿彬, 陈仲清. VA-ECMO患者院内死亡风险预测模型的构建及验证:一项多中心、回顾性、病例对照研究[J]. 南方医科大学学报, 2024, 44(3): 491-498. |
| [3] | 刘云泽, 李宬润, 郭俊唐, 刘 阳. 基于临床-影像组学列线图模型鉴别局灶性机化性肺炎与肺腺癌[J]. 南方医科大学学报, 2024, 44(2): 397-404. |
| [4] | 张奔龙, 鲁意迅, 李 力, 高云鹤, 梁文全, 郗洪庆, 王鑫鑫, 张珂诚, 陈 凛. 基于单中心490例胃神经内分泌肿瘤建立的列线图具有良好的预后预测性能[J]. 南方医科大学学报, 2023, 43(2): 183-190. |
| [5] | 张浩轩, 陆 进, 蒋成义, 方美芳. 基于人工智能技术的鼻咽癌风险预测模型的构建与评价[J]. 南方医科大学学报, 2023, 43(2): 271-279. |
| [6] | 孔德贤, 宋丽萍, 向 阳. PET/CT代谢参数与血液炎症标志物对一线化疗的非小细胞肺癌患者预后列线图的构建及临床意义[J]. 南方医科大学学报, 2023, 43(12): 2139-2144. |
| [7] | 刘昭君, 周晓莉. 基于系统性炎症指标构建的列线图可预测心力衰竭患者的不良结局[J]. 南方医科大学学报, 2022, 42(8): 1149-1158. |
| [8] | 罗 钞, 王高明, 胡力文, 强 勇, 郑 超, 申 翼. 食管癌患者术后预测模型的构建和验证:基于SEER数据库[J]. 南方医科大学学报, 2022, 42(6): 794-804. |
| [9] | 孟令飞, 朱学研, 杨立明, 李忻阳, 程思宇, 郭师正, 庄小花, 邹洪斌, 崔文鹏. 腹膜透析相关腹膜炎患者治疗失败预测模型的构建和验证:一项多中心临床研究[J]. 南方医科大学学报, 2022, 42(4): 546-553. |
| [10] | 邓 亚, 王春艳, 付懿铭, 李忠斌, 纪 冬. 慢性药物性肝损伤的复发风险与肝纤维化程度高度相关[J]. 南方医科大学学报, 2022, 42(11): 1655-1661. |
| [11] | 赵晨玲, 董 婷, 孙伦燕, 胡慧冰, 王 琼, 田丽伟, 江张胜. Wilson病脂代谢异常患者发生肝纤维化的列线图预测模型的建立与验证[J]. 南方医科大学学报, 2022, 42(11): 1720-1725. |
| [12] | 蔡 虹, 刘 勉, 林妙玲, 李 红, 沈 朗, 全 松. CCN5在子宫内膜异位症患者组织的表达及其作用机制[J]. 南方医科大学学报, 2022, 42(1): 86-92. |
| [13] | 聂伟哲, 李舒婷, Krina T. Zondervan, Christian M. Becker, 郭逸男, 宗利丽. 中国和英国子宫内膜异位症患者的发病相关因素分析[J]. 南方医科大学学报, 2022, 42(1): 137-142. |
| [14] | 张海捷, 殷 夫, 陈梦林, 漆安琪, 杨丽洋, 崔维维, 杨姗姗, 文 戈. 基于术前CT影像组学列线图可预测Ⅰ~Ⅲ期肾透明性细胞癌术后复发[J]. 南方医科大学学报, 2021, 41(9): 1358-1365. |
| [15] | 曹众平, 熊习安, 杨 群. 朴素贝叶斯分类器在化疗所致恶心呕吐风险预测模型上的应用[J]. 南方医科大学学报, 2021, 41(4): 607-612. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||