南方医科大学学报 ›› 2024, Vol. 44 ›› Issue (5): 989-997.doi: 10.12122/j.issn.1673-4254.2024.05.22
申磊磊1( ), 陈莹1(), 云天洋1, 郭俊唐2, 柳曦2, 张涛2, 梁朝阳2, 刘阳2()
), 陈莹1(), 云天洋1, 郭俊唐2, 柳曦2, 张涛2, 梁朝阳2, 刘阳2()
收稿日期:2023-11-12
出版日期:2024-05-20
发布日期:2024-06-06
通讯作者:
刘阳
E-mail:drshenats@163.com;15692537361@163.com;sunny301x@sina.com
作者简介:申磊磊,博士,主治医师,E-mail: drshenats@163.com
Leilei SHEN1(), Ying CHEN1(), Tianyang YUN1, Juntang GUO2, Xi LIU2, Tao ZHANG2, Chaoyang LIANG2, Yang LIU2()
Received:2023-11-12
Online:2024-05-20
Published:2024-06-06
Contact:
Yang LIU
E-mail:drshenats@163.com;15692537361@163.com;sunny301x@sina.com
摘要:
目的 探索ⅠB期肺腺癌患者的辅助治疗方案。 方法 收集2013年1月~2021年12月在我院行手术治疗的IB期肺腺癌患者,根据术后不同辅助治疗模式分为辅助靶向治疗组(EGFR-TKIs)、辅助化疗组(CT)和临床观察组(CO)。对比3组患者的临床资料和随访结果,无疾病生存期、总生存的分析采用Kaplan-Meier法并行log-rank检验,COX回归分析患者无疾病生存期(DFS)的预测因素。主要研究终点是5年DFS率,次要研究终点为DFS、3年总生存期(OS)以及辅助治疗的安全性。 结果 共纳入653例术后诊断为IB期肺腺癌患者,其中EGFR-TKIs组111例,CT组108例,CO组434例。中位随访时间43个月,TKIs组、CT组和CO组的5年DFS率分别为92.8%、80.7%及81.7%,TKIs组的5年DFS率显著高于CO组(P<0.01)。TKIs组、CT组和CO组的3年OS均无统计学差异。亚组分析显示,T3~4 cmN0M0中TKIs组、CT组和CO组的5年DFS率分别为92.6%、84.0%及81.4%,TKIs组的5年DFS率显著高于CO组(P<0.05),3组间的3年OS无统计学差异。而T2ViscPlN0M0中TKIs组、CT组和CO组的5年DFS率分别为95.1%、71.4%及83.5%,组间差异并无统计学意义,3组间的3年OS亦无统计学差异。多因素COX回归分析结果显示,年龄(P<0.05;HR 0.631,95% CI 0.401-0.993)、实性结节(P<0.01;HR 7.620,95% CI 3.037-19.121)、微乳头/实性成分(P<0.05;HR 1.776,95% CI 1.010-3.122)、脉管癌栓(P<0.05;HR 2.981,95% CI 1.198-7.419)及辅助治疗(P<0.01)是DFS的独立预测因素。安全性方面,皮疹、甲沟炎及腹泻仍然是靶向药物最常见的不良反应。化疗组不良反应主要为血液系统的抑制和胃肠道反应,3级以上不良反应率高于TKIs组(44.4% vs 9.0%)。 结论 辅助靶向治疗有助于提高T3~4 cmN0M0的IB期肺腺癌患者的DFS,但T2ViscPlN0M0患者并不能从靶向治疗中获益。辅助化疗并不能改善IB期肺腺癌患者的DFS和OS。
申磊磊, 陈莹, 云天洋, 郭俊唐, 柳曦, 张涛, 梁朝阳, 刘阳. IB期肺腺癌患者辅助治疗方案的筛选[J]. 南方医科大学学报, 2024, 44(5): 989-997.
Leilei SHEN, Ying CHEN, Tianyang YUN, Juntang GUO, Xi LIU, Tao ZHANG, Chaoyang LIANG, Yang LIU. Selection of postoperative adjuvant therapy for patients with stage IB lung adenocarcinoma: analysis of 653 cases[J]. Journal of Southern Medical University, 2024, 44(5): 989-997.
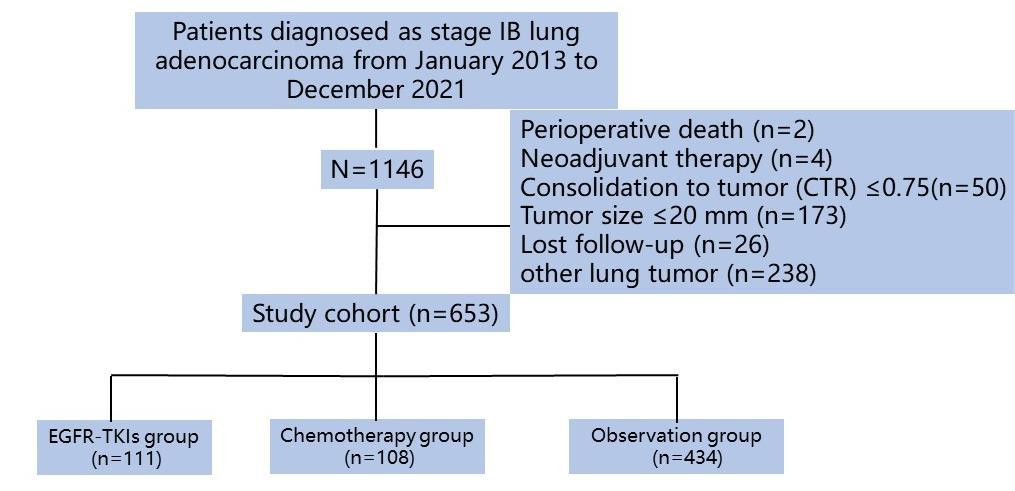
图1 研究流程图
Fig.1 Flow diagram of patient enrollment.
| Characteristic No. | TKIs group (n=111) | CT group (n=108) | CO group (n=434) | P |
|---|---|---|---|---|
| Gender | 0.003 | |||
| Male | 38 (34.2)* # | 57 (52.8) | 226 (52.1) | |
| Female | 73 (65.8)* # | 51 (47.2) | 208 (47.9) | |
| Age (year) | 60.66±9.05* | 57.45±9.07 # | 61.08±8.95 | 0.001 |
| ≤65 | 72 (64.9)* | 88 (81.5) # | 287 (66.1) | 0.006 |
| >65 | 39 (35.1)* | 20 (18.5) # | 147 (33.9) | 0.006 |
| Smoking history | 26 (23.4) | 40 (37.0) | 135 (31.1) | 0.091 |
| Family history of lung cancer | 16 (14.4) | 12 (11.1) | 47 (10.8) | 0.584 |
| CEA abnormality | 18 (16.2) # | 9 (8.3) | 33 (7.6) | 0.019 |
| Diabetes mellitus | 7 (6.3) | 7 (6.5) | 51 (11.8) | 0.096 |
| Hypertension | 31 (27.9) | 22 (20.4) | 121 (27.9) | 0.280 |
| Cardiovascular disease | 8 (7.2) | 5 (4.6) | 26 (6.0) | 0.687 |
| Cerebrovascular disease | 4 (3.6) | 2 (1.9) | 14 (3.2) | 0.797 |
| PET-CT | 8.00 (3.60, 10.00) | 6.85 (3.13, 9.00) | 4.85 (2.20, 8.60) | 0.175 |
| Tumor location | 0.154 | |||
| RUL | 34 (30.6) | 34 (31.5) | 139 (32.0) | |
| RML | 14 (12.6) | 5 (4.6) | 31 (7.1) | |
| RLL | 11(9.9) | 22 (20.4) | 79 (18.2) | |
| LUL | 30 (27.0) | 32 (29.6) | 104 (24.0) | |
| LLL | 22 (19.8) | 15 (13.9) | 81 (18.78) | |
| CTR | 1 (1, 1) | 1 (1, 1) | 1 (0.87, 1) | 0.105 |
| Solid nodule | 71 (64.0) | 81 (75.0) # | 271 (62.4) | 0.049 |
| Surgical procedure | 0.412 | |||
| Sublobectomy | 15 (13.5) | 9 (8.3) | 43 (9.9) | |
| Lobectomy | 96 (86.5) | 99 (91.7) | 391 (90.1) | |
| LND | ||||
| Stations | 5 (5, 6) | 5.5 (3.25, 6) | 5 (4, 6) | 0.859 |
| Numbers | 9 (6, 16) | 9.5 (4.5, 16) | 10 (7, 16) | 0.507 |
| pNx | 30 (27.0) | 30 (27.8) | 114 (26.3) | 0.956 |
表1 肺腺癌患者临床基线资料
Tab.1 Baseline clinical characteristics of the patients with adenocarcinoma in the 3 groups
| Characteristic No. | TKIs group (n=111) | CT group (n=108) | CO group (n=434) | P |
|---|---|---|---|---|
| Gender | 0.003 | |||
| Male | 38 (34.2)* # | 57 (52.8) | 226 (52.1) | |
| Female | 73 (65.8)* # | 51 (47.2) | 208 (47.9) | |
| Age (year) | 60.66±9.05* | 57.45±9.07 # | 61.08±8.95 | 0.001 |
| ≤65 | 72 (64.9)* | 88 (81.5) # | 287 (66.1) | 0.006 |
| >65 | 39 (35.1)* | 20 (18.5) # | 147 (33.9) | 0.006 |
| Smoking history | 26 (23.4) | 40 (37.0) | 135 (31.1) | 0.091 |
| Family history of lung cancer | 16 (14.4) | 12 (11.1) | 47 (10.8) | 0.584 |
| CEA abnormality | 18 (16.2) # | 9 (8.3) | 33 (7.6) | 0.019 |
| Diabetes mellitus | 7 (6.3) | 7 (6.5) | 51 (11.8) | 0.096 |
| Hypertension | 31 (27.9) | 22 (20.4) | 121 (27.9) | 0.280 |
| Cardiovascular disease | 8 (7.2) | 5 (4.6) | 26 (6.0) | 0.687 |
| Cerebrovascular disease | 4 (3.6) | 2 (1.9) | 14 (3.2) | 0.797 |
| PET-CT | 8.00 (3.60, 10.00) | 6.85 (3.13, 9.00) | 4.85 (2.20, 8.60) | 0.175 |
| Tumor location | 0.154 | |||
| RUL | 34 (30.6) | 34 (31.5) | 139 (32.0) | |
| RML | 14 (12.6) | 5 (4.6) | 31 (7.1) | |
| RLL | 11(9.9) | 22 (20.4) | 79 (18.2) | |
| LUL | 30 (27.0) | 32 (29.6) | 104 (24.0) | |
| LLL | 22 (19.8) | 15 (13.9) | 81 (18.78) | |
| CTR | 1 (1, 1) | 1 (1, 1) | 1 (0.87, 1) | 0.105 |
| Solid nodule | 71 (64.0) | 81 (75.0) # | 271 (62.4) | 0.049 |
| Surgical procedure | 0.412 | |||
| Sublobectomy | 15 (13.5) | 9 (8.3) | 43 (9.9) | |
| Lobectomy | 96 (86.5) | 99 (91.7) | 391 (90.1) | |
| LND | ||||
| Stations | 5 (5, 6) | 5.5 (3.25, 6) | 5 (4, 6) | 0.859 |
| Numbers | 9 (6, 16) | 9.5 (4.5, 16) | 10 (7, 16) | 0.507 |
| pNx | 30 (27.0) | 30 (27.8) | 114 (26.3) | 0.956 |
| Characteristic | TKIs group (n=111) | CT group (n=108) | CO group (n=434) | P |
|---|---|---|---|---|
| Tumor diameter(mm) | 30.89±5.87 | 32.10±6.23 # | 29.74±5.80 | 0.001 |
| >3 cm | 68 (61.3) | 75 (69.4) | 260 (59.9) | 0.192 |
| ≤3 cm | 43 (38.7) | 33 (30.6) | 174 (40.1) | 0.192 |
| ≥1 high-risk factors | 105 (94.6) | 102 (94.4) | 397 (91.5) | 0.389 |
| Mucous component | 8 (7.2) | 11 (10.3) | 35 (8.1) | 0.706 |
| Micropapillary or solid component | 50(45.0)* | 67 (62.0) # | 154 (35.5) | <0.001 |
| VPI | 82 (73.9) | 88 (81.5) | 333 (76.7) | 0.397 |
| LVI | 7 (6.3) # | 9 (8.3) # | 7 (1.6) | <0.001 |
| STAS | 12 (10.8) # | 11 (10.2) # | 19 (4.4) | 0.011 |
| Ki-67 index(≥20%) | 36 (42.9) | 40 (44.9) | 120 (36.8) | 0.289 |
| EGFR mutation | 111 (100)* # | 18/44 (40.9) # | 78/110 (70.9) | <0.001 |
| 19 del | 52/111 (46.8) | 5/18 (27.8) | 31/78 (39.7) | - |
| 21 L858R | 58/111 (52.2) | 8/18 (44.4) | 41/78 (52.5) | - |
| 20 T790M/20 ins | 0/0 | 0/3 | 1/2 | - |
| G719X/S861I/L861Q | 1/0/0 | 1/0/1 | 1/1/1 | - |
| ALK mutation | 0* # | 4/40 (10) | 9/101 (8.9) | 0.011 |
| KRAS mutation | 1/48 (2.0) | 4/37 (10.8) | 7/88 (7.9) | 0.252 |
| TP53 mutation | 9/26 (34.6) | 8/20 (40) | 15/46 (32.6) | 0.893 |
| PD-L1 | 0 (0, 5) | 1.5 (0, 5) | 0 (0, 3) | 0.240 |
| IASLC grade | 0.002 | |||
| 1 | 9 (8.1) # | 4 (3.7) # | 23 (5.3) | |
| 2 | 66 (59.5) # | 50 (46.3) # | 280 (64.5) | |
| 3 | 36 (32.4) # | 54 (50.0) # | 131 (30.2) |
表2 肺腺癌患者病理资料
Tab.2 Pathological findings of the patients with adenocarcinoma in the 3 groups
| Characteristic | TKIs group (n=111) | CT group (n=108) | CO group (n=434) | P |
|---|---|---|---|---|
| Tumor diameter(mm) | 30.89±5.87 | 32.10±6.23 # | 29.74±5.80 | 0.001 |
| >3 cm | 68 (61.3) | 75 (69.4) | 260 (59.9) | 0.192 |
| ≤3 cm | 43 (38.7) | 33 (30.6) | 174 (40.1) | 0.192 |
| ≥1 high-risk factors | 105 (94.6) | 102 (94.4) | 397 (91.5) | 0.389 |
| Mucous component | 8 (7.2) | 11 (10.3) | 35 (8.1) | 0.706 |
| Micropapillary or solid component | 50(45.0)* | 67 (62.0) # | 154 (35.5) | <0.001 |
| VPI | 82 (73.9) | 88 (81.5) | 333 (76.7) | 0.397 |
| LVI | 7 (6.3) # | 9 (8.3) # | 7 (1.6) | <0.001 |
| STAS | 12 (10.8) # | 11 (10.2) # | 19 (4.4) | 0.011 |
| Ki-67 index(≥20%) | 36 (42.9) | 40 (44.9) | 120 (36.8) | 0.289 |
| EGFR mutation | 111 (100)* # | 18/44 (40.9) # | 78/110 (70.9) | <0.001 |
| 19 del | 52/111 (46.8) | 5/18 (27.8) | 31/78 (39.7) | - |
| 21 L858R | 58/111 (52.2) | 8/18 (44.4) | 41/78 (52.5) | - |
| 20 T790M/20 ins | 0/0 | 0/3 | 1/2 | - |
| G719X/S861I/L861Q | 1/0/0 | 1/0/1 | 1/1/1 | - |
| ALK mutation | 0* # | 4/40 (10) | 9/101 (8.9) | 0.011 |
| KRAS mutation | 1/48 (2.0) | 4/37 (10.8) | 7/88 (7.9) | 0.252 |
| TP53 mutation | 9/26 (34.6) | 8/20 (40) | 15/46 (32.6) | 0.893 |
| PD-L1 | 0 (0, 5) | 1.5 (0, 5) | 0 (0, 3) | 0.240 |
| IASLC grade | 0.002 | |||
| 1 | 9 (8.1) # | 4 (3.7) # | 23 (5.3) | |
| 2 | 66 (59.5) # | 50 (46.3) # | 280 (64.5) | |
| 3 | 36 (32.4) # | 54 (50.0) # | 131 (30.2) |
| Distribution | Icotinib (n=65) | Gefitinib (n=28) | Furmonertinib/ almonertinib (n=1/2) | Osimertinib (n=15) | Chemotherapy (n=108) |
|---|---|---|---|---|---|
| Duration | |||||
| 1 year/2 cycles | 25 (38.5) | 6 (21.4) | 1 (33) | 3 (20) | 6 (5.6) |
| 2 years/3 cycles | 36 (55.4) | 16 (57.1) | 2 (66) | 12 (80) | 8 (7.4) |
| 3 years/4 cycles | 2 (3.1) | 5 (17.9) | 0 | 0 | 94 (87) |
| 5 years | 2 (3.1) | 1 (3.6) | 0 | 0 | - |
| Economy cost (RMB/year) | 3.9×104 | 1.4×104 | Not applicable | 6.4×104 | Not applicable |
| Adverse events | |||||
| Rash | 24 (36.9) | 11 (40) | 2 (66) | 3 (20) | 0 |
| Paronychia | 11 (16.9) | 7 (25) | 1 (33) | 4 (26.7) | 0 |
| Interstitial pneumonia | 0 | 0 | 0 | 0 | 0 |
| Thrombocytopenia | 1 (1.5) | 1 (3.6) | 0 | 1 (1.5) | 21 (19.4) |
| Leukopenia | 1 (1.5) | 1 (3.6) | 0 | 1 (1.5) | 64 (59.3) |
| Diarrhea | 13 (20) | 6 (30) | 1 (33) | 6 (40) | 5 (4.6) |
| Nausea | 2 (3) | 2 (7.1) | 0 | 3 (20) | 60 (55.6) |
| Decreased appetite | 1 (1.5) | 1 (3.6) | 1 (33) | 2 (13.3) | 20 (18.5) |
| Grade ≥3 | 5 (7.7) | 4 (14.3) | 0 | 1 (6.5) | 48 (44.4) |
表3 辅助治疗药物的分布及安全情况
Tab.3 Adjuvant therapy and adverse events in the 3 groups
| Distribution | Icotinib (n=65) | Gefitinib (n=28) | Furmonertinib/ almonertinib (n=1/2) | Osimertinib (n=15) | Chemotherapy (n=108) |
|---|---|---|---|---|---|
| Duration | |||||
| 1 year/2 cycles | 25 (38.5) | 6 (21.4) | 1 (33) | 3 (20) | 6 (5.6) |
| 2 years/3 cycles | 36 (55.4) | 16 (57.1) | 2 (66) | 12 (80) | 8 (7.4) |
| 3 years/4 cycles | 2 (3.1) | 5 (17.9) | 0 | 0 | 94 (87) |
| 5 years | 2 (3.1) | 1 (3.6) | 0 | 0 | - |
| Economy cost (RMB/year) | 3.9×104 | 1.4×104 | Not applicable | 6.4×104 | Not applicable |
| Adverse events | |||||
| Rash | 24 (36.9) | 11 (40) | 2 (66) | 3 (20) | 0 |
| Paronychia | 11 (16.9) | 7 (25) | 1 (33) | 4 (26.7) | 0 |
| Interstitial pneumonia | 0 | 0 | 0 | 0 | 0 |
| Thrombocytopenia | 1 (1.5) | 1 (3.6) | 0 | 1 (1.5) | 21 (19.4) |
| Leukopenia | 1 (1.5) | 1 (3.6) | 0 | 1 (1.5) | 64 (59.3) |
| Diarrhea | 13 (20) | 6 (30) | 1 (33) | 6 (40) | 5 (4.6) |
| Nausea | 2 (3) | 2 (7.1) | 0 | 3 (20) | 60 (55.6) |
| Decreased appetite | 1 (1.5) | 1 (3.6) | 1 (33) | 2 (13.3) | 20 (18.5) |
| Grade ≥3 | 5 (7.7) | 4 (14.3) | 0 | 1 (6.5) | 48 (44.4) |
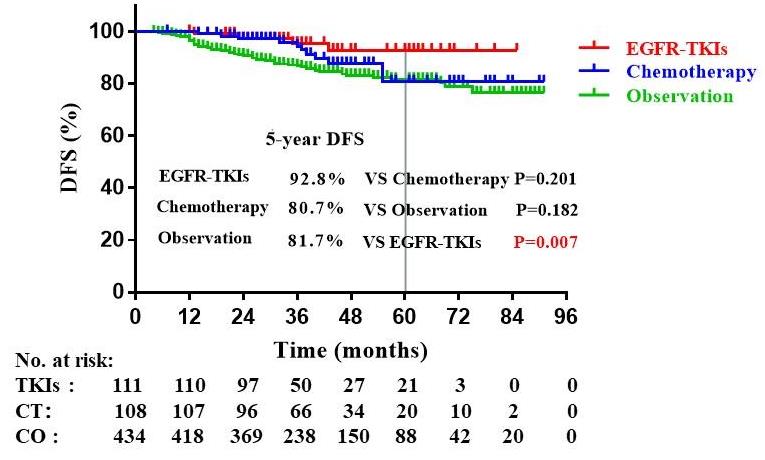
图2 全队列患者DFS生存曲线
Fig.2 Kaplan-Meier curve for DFS of the entire cohort.
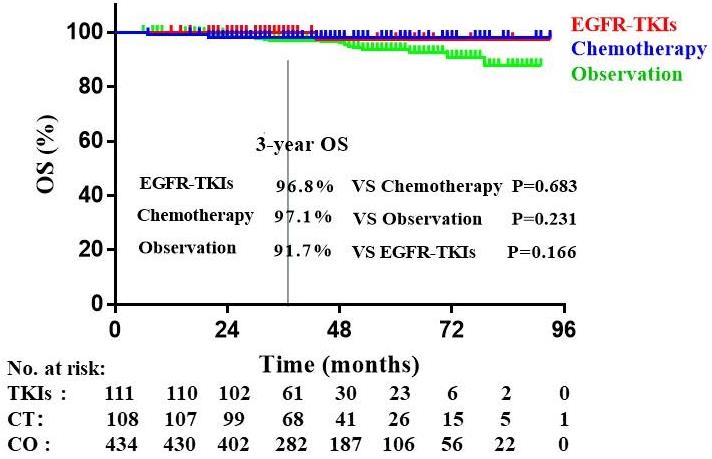
图3 全队列患者OS生存曲线
Fig 3 Kaplan-Meier curve for OS of the entire cohort.
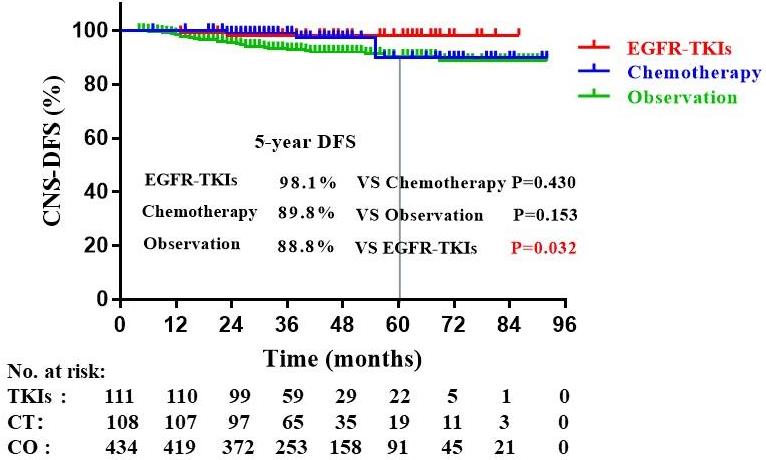
图4 全队列患者CNS-DFS生存曲线
Fig.4 Kaplan-Meier curve for CNS-DFS of the entire cohort.
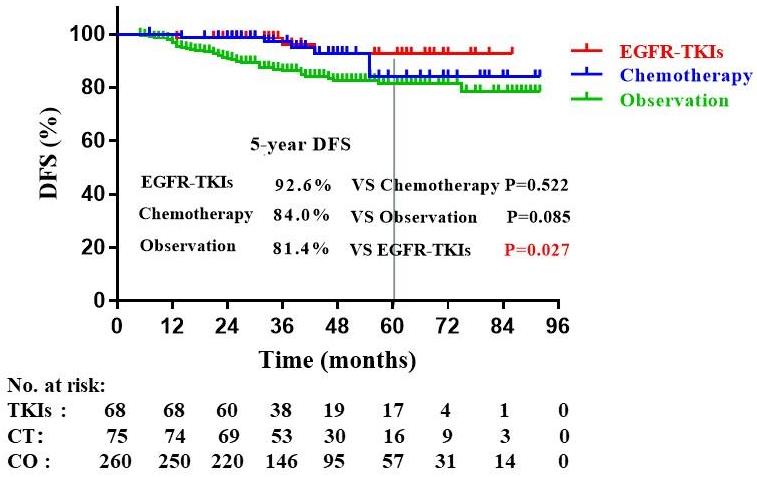
图5 T3~4 cm N0M0患者DFS生存曲线
Fig.5 Kaplan-Meier curve for DFS of T3-4cmN0M0 patients.
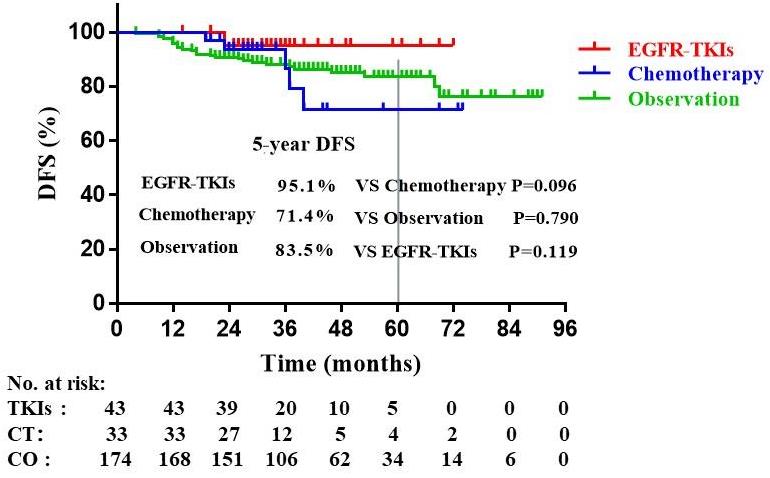
图6 T2ViscPlN0M0患者DFS生存曲线
Fig.6 Kaplan-Meier curve for DFS of T2ViscPlN0M0 patients.
| DFS predictor | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Age (≤65 year) | 1.028 (1.003-1.053) | 0.030 | 0.631 (0.401- 0.993) | 0.046 |
| Gender | 1.774 (1.135-2.772) | 0.012 | 1.325 (0.830-2.117) | 0.238 |
| Solid nodule | 7.777 (3.386-17.859) | <0.001 | 7.620 (3.037-19.121) | <0.001 |
| CTR | 1.002 (1-1.005) | 0.040 | 1.014 (0.879-1.170) | 0.849 |
| IASLC grade 3 | Reference | 0.004 | Reference | 0.945 |
| 1 | 4.291 (0.590-31.182) | 0.150 | - | 0.881 |
| 2 | 8.085 (1.11-58.884) | 0.039 | - | 0.882 |
| Micropapillary or solid component | 2.476 (1.589-3.859) | <0.001 | 1.776 (1.010-3.122) | 0.046 |
| STAS | 2.665 (1.369-5.187) | 0.004 | 1.866 (0.924- 3.766) | 0.082 |
| LVI | 2.995 (1.3-6.9) | 0.010 | 2.981 (1.198-7.419) | 0.019 |
| pNx | 1.639 (1.049-2.562) | 0.030 | 1.4557 (0.977-2.481) | 0.062 |
| Adjuvant therapy | 0.023 | 0.002 | ||
| EGFR-TKIs | 0.308 (0.124-0.765) | 0.011 | 0.257 (0.102-0.646) | 0.004 |
| Chemotherapy | 0.655 (0.346-1.239) | 0.193 | 0.414 (0.207-0.827) | 0.012 |
表4 DFS预后因素的单因素和多因素COX回归分析
Tab.4 Univariate and Multivariate Cox Regression Analysis of DFS factors
| DFS predictor | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Age (≤65 year) | 1.028 (1.003-1.053) | 0.030 | 0.631 (0.401- 0.993) | 0.046 |
| Gender | 1.774 (1.135-2.772) | 0.012 | 1.325 (0.830-2.117) | 0.238 |
| Solid nodule | 7.777 (3.386-17.859) | <0.001 | 7.620 (3.037-19.121) | <0.001 |
| CTR | 1.002 (1-1.005) | 0.040 | 1.014 (0.879-1.170) | 0.849 |
| IASLC grade 3 | Reference | 0.004 | Reference | 0.945 |
| 1 | 4.291 (0.590-31.182) | 0.150 | - | 0.881 |
| 2 | 8.085 (1.11-58.884) | 0.039 | - | 0.882 |
| Micropapillary or solid component | 2.476 (1.589-3.859) | <0.001 | 1.776 (1.010-3.122) | 0.046 |
| STAS | 2.665 (1.369-5.187) | 0.004 | 1.866 (0.924- 3.766) | 0.082 |
| LVI | 2.995 (1.3-6.9) | 0.010 | 2.981 (1.198-7.419) | 0.019 |
| pNx | 1.639 (1.049-2.562) | 0.030 | 1.4557 (0.977-2.481) | 0.062 |
| Adjuvant therapy | 0.023 | 0.002 | ||
| EGFR-TKIs | 0.308 (0.124-0.765) | 0.011 | 0.257 (0.102-0.646) | 0.004 |
| Chemotherapy | 0.655 (0.346-1.239) | 0.193 | 0.414 (0.207-0.827) | 0.012 |
| 1 | 郑荣寿, 孙可欣, 张思维, 等. 2015年中国恶性肿瘤流行情况分析[J]. 中华肿瘤杂志, 2019, 41(1): 19-28. |
| 2 | Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2022[J]. CA A Cancer J Clinicians, 2022, 72(1): 7-33. DOI: 10.3322/caac.21708 |
| 3 | Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE collaborative group[J]. J Clin Oncol, 2008, 26(21): 3552-9. DOI: 10.1200/jco.2007.13.9030 |
| 4 | Wu YL, iMTsubo, He J, et al. Osimertinib in Resected EGFR-mutated non-small-cell lung cancer[J]. N Engl J Med, 2020, 383(18):1711-23. |
| 5 | Winton T, Livingston R, Johnson D, et al. Vinorelbine plus cisplatin vs. observation in resected non-small-cell lung cancer[J]. N Engl J Med, 2005, 352(25): 2589-97. DOI: 10.1056/nejmoa043623 |
| 6 | Arriagada R, Bergman B, Dunant A, et al. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer[J]. N Engl J Med, 2004, 350(4): 351-60. DOI: 10.1056/nejmoa031644 |
| 7 | Douillard JY, Rosell R, De Lena M, et al. Adjuvant vinorelbine plus cisplatin versus observation in patients with completely resected stage IB-IIIA non-small-cell lung cancer (Adjuvant Navelbine International Trialist Association[ANITA]): a randomised controlled trial[J]. Lancet Oncol, 2006, 7(9): 719-27. DOI: 10.1016/s1470-2045(06)70804-x |
| 8 | Scagliotti GV, Fossati R, Torri V, et al. Randomized study of adjuvant chemotherapy for completely resected stage I, II, or IIIA non-small-cell Lung cancer[J]. J Natl Cancer Inst, 2003, 95(19): 1453-61. DOI: 10.1093/jnci/djg059 |
| 9 | Waller D, Peake MD, Stephens RJ, et al. Chemotherapy for patients with non-small cell lung cancer: the surgical setting of the Big Lung Trial[J]. Eur J Cardiothorac Surg, 2004, 26(1): 173-82. DOI: 10.1016/j.ejcts.2004.03.041 |
| 10 | Remon J, Soria JC, Peters S, et al. Early and locally advanced non-small-cell lung cancer: an update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging, systemic and local therapy[J]. Ann Oncol, 2021, 32(12): 1637-42. DOI: 10.1016/j.annonc.2021.08.1994 |
| 11 | Kris MG, Gaspar LE, Chaft JE, et al. Adjuvant systemic therapy and adjuvant radiation therapy for stage I to IIIA completely resected non-small-cell lung cancers: American society of clinical oncology/cancer care Ontario clinical practice guideline update[J]. J Clin Oncol, 2017, 35(25): 2960-74. DOI: 10.1200/jco.2017.72.4401 |
| 12 | 中国临床肿瘤学会指南工作委员会组织. 中国临床肿瘤学会(CSCO)非小细胞肺癌诊疗指南-2023[M]. 北京:人民卫生出版社, 2023. |
| 13 | Ettinger DS, Wood DE, Aisner DL, et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology[J]. J Natl Compr Canc Netw, 2022,20(5):497-530. |
| 14 | Tsuboi M, Herbst RS, John T, et al. Overall survival with osimertinib in resected EGFR-mutated NSCLC[J]. N Engl J Med, 2023, 389(2): 137-47. DOI: 10.1056/nejmoa2304594 |
| 15 | Zhong WZ, Wang Q, Mao WM, et al. Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II-IIIA (N1-N2) EGFR-mutant NSCLC (ADJUVANT/CTONG1104): a randomised, open-label, phase 3 study[J]. Lancet Oncol, 2018, 19(1): 139-48. DOI: 10.1016/s1470-2045(17)30729-5 |
| 16 | Yue D, Xu S, Wang Q, et al. Erlotinib versus vinorelbine plus cisplatin as adjuvant therapy in Chinese patients with stage ⅢA EGFR mutation-positive non-small-cell lung cancer (EVAN): a randomised, open‐label, phase 2 trial[J]. Lancet Respir Med, 2018, 6(11): 863‐73. DOI: 10.1016/s2213-2600(18)30277-7 |
| 17 | He JX, Su CX, Liang WH, et al. Icotinib versus chemotherapy as adjuvant treatment for stage II-IIIA EGFR-mutant non-small-cell lung cancer (EVIDENCE): a randomised, open-label, phase 3 trial[J]. Lancet Respir Med, 2021, 9(9): 1021-9. DOI: 10.1016/s2213-2600(21)00134-x |
| 18 | Ou W, Li N, Wang BX, et al. Adjuvant icotinib versus observation in patients with completely resected EGFR-mutated stage IB NSCLC (GASTO1003, CORIN): a randomised, open-label, phase 2 trial[J]. EClinicalMedicine, 2023, 57: 101839. DOI: 10.1016/j.eclinm.2023.101839 |
| 19 | Shen LL, Guo JT, Zhang WD, et al. Clinical efficacy and safety of adjuvant EGFR-TKIs for resected stage IB lung adenocarcinoma: a real-world study based on propensity score matching[J]. Cancer Med, 2023, 12(18): 18470-8. DOI: 10.1002/cam4.6443 |
| 20 | Detterbeck FC, Boffa DJ, Kim AW, et al. The eighth edition lung cancer stage classification[J]. Chest, 2017, 151(1): 193-203. DOI: 10.1016/j.chest.2016.10.010 |
| 21 | Bankier AA, MacMahon H, Goo JM, et al. Recommendations for measuring pulmonary nodules at CT: a statement from the fleischner society[J]. Radiology, 2017, 285(2): 584-600. DOI: 10.1148/radiol.2017162894 |
| 22 | Travis WD, Brambilla E, Noguchi M, et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society: international multidisciplinary classification of lung adenocarcinoma: executive summary[J]. Proc Am Thorac Soc, 2011, 8(5): 381-5. DOI: 10.1513/pats.201107-042st |
| 23 | Nicholson AG, Tsao MS, Beasley MB, et al. The 2021 WHO classification of lung tumors: impact of advances since 2015[J]. J Thorac Oncol, 2022, 17(3): 362-87. DOI: 10.1016/j.jtho.2021.11.003 |
| 24 | Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0 [S]. . DOI: 10.1016/b978-032303978-9.50028-9 |
| 25 | Strauss GM, Wang XF, Maddaus M, et al. Adjuvant chemotherapy (AC) in stage IB non-small cell lung cancer (NSCLC): long-term follow-up of Cancer and Leukemia Group B (CALGB) 9633[J]. J Clin Oncol, 2011, 29(): 7015. DOI: 10.1200/jco.2011.29.15_suppl.7015 |
| 26 | Wang XF, Chen DL, Wen JM, et al. Benefit of adjuvant chemotherapy for patients with stage IB non-small cell lung cancer: a systematic review and meta-analysis[J]. Ann Transl Med, 2021, 9(18): 1430. DOI: 10.21037/atm-21-4001 |
| 27 | Casiraghi M, Petrella F, Bardoni C, et al. Surgically treated pT2aN0M0 (stage IB) non-small cell lung cancer: a 20-year single-center retrospective study[J]. J Clin Med, 2023, 12(5): 2081. DOI: 10.3390/jcm12052081 |
| 28 | Lee PH, Chiang CJ, Tseng JS, et al. Adjuvant chemotherapy compared with observation in patients with T2aN0 stage IB lung adenocarcinoma[J]. Front Oncol, 2023, 13: 1096683. DOI: 10.3389/fonc.2023.1096683 |
| 29 | Rami-Porta R, Bolejack V, Crowley J, et al. The IASLC lung cancer staging project: proposals for the revisions of the T descriptors in the forthcoming eighth edition of the TNM classification for lung cancer[J]. J Thorac Oncol, 2015, 10(7): 990-1003. DOI: 10.1097/jto.0000000000000559 |
| 30 | Liang RB, Li P, Li BT, et al. Modification of pathologic T classification for non-small cell lung cancer with visceral pleural invasion: data from 1, 055 cases of cancers≤3 cm[J]. Chest, 2021, 160(2): 754-64. DOI: 10.1016/j.chest.2021.03.022 |
| 31 | Huang WJ, Deng HY, Lin MY, et al. Treatment modality for stage IB peripheral non-small cell lung cancer with visceral pleural invasion and ≤3 cm in size[J]. Front Oncol, 2022, 12: 830470. DOI: 10.3389/fonc.2022.830470 |
| 32 | Pathak R, Goldberg SB, Canavan M, et al. Association of survival with adjuvant chemotherapy among patients with early-stage non-small cell lung cancer with vs without high-risk clinicopathologic features[J]. JAMA Oncol, 2020, 6(11): 1741-50. DOI: 10.1001/jamaoncol.2020.4232 |
| 33 | Yang ZJ, Li XF, Bai JS, et al. Prognostic factors for survival of stage IB non-small cell lung cancer patients: a 10-year follow-up retrospective study[J]. Ann Surg Oncol, 2023, 30(12): 7481-91. DOI: 10.1245/s10434-023-14016-y |
| 34 | Chen DL, Wang XF, Zhang FQ, et al. Could tumor spread through air spaces benefit from adjuvant chemotherapy in stage I lung adenocarcinoma? A multi-institutional study[J]. Ther Adv Med Oncol, 2020, 12: 1758835920978147. DOI: 10.1177/1758835920978147 |
| 35 | Qian FF, Yang WJ, Wang R, et al. Prognostic significance and adjuvant chemotherapy survival benefits of a solid or micropapillary pattern in patients with resected stage IB lung adenocarcinoma[J]. J Thorac Cardiovasc Surg, 2018, 155(3): 1227-35. e2. DOI: 10.1016/j.jtcvs.2017.09.143 |
| [1] | 刘云泽, 李宬润, 郭俊唐, 刘 阳. 基于临床-影像组学列线图模型鉴别局灶性机化性肺炎与肺腺癌[J]. 南方医科大学学报, 2024, 44(2): 397-404. |
| [2] | 王会杰, 孙珍贵, 赵文英, 耿 彪. S100A10可促进肺腺癌细胞的增殖和侵袭:基于激活Akt-mTOR信号通路[J]. 南方医科大学学报, 2023, 43(5): 733-740. |
| [3] | 黄云龙, 朱玉峰, 石 瑾, 刘 蓉, 曾 婷, 韩良辅. β-羟基丁酸抑制肺腺癌细胞增殖、迁移及侵袭的作用机制[J]. 南方医科大学学报, 2023, 43(10): 1744-1751. |
| [4] | 洪海宁, 朱浩楠, 李 超, 臧 超, 桑海威, 陈力维, 王安生. FNDC1在肺腺癌中高表达并与不良预后相关[J]. 南方医科大学学报, 2022, 42(8): 1182-1190. |
| [5] | 陈文邦, 朱 潇, 周 少, 杏福宝, 唐 震, 李小军, 张 雷. 敲低galectin-1可抑制肺腺癌细胞的增殖、迁移和侵袭并促进其凋亡[J]. 南方医科大学学报, 2022, 42(11): 1628-1637. |
| [6] | 廖 晖, 王 毅, 徐小平, 周陈杰, 张健民, 钟克波, 杨定华. 双mTORC1/2抑制剂AZD2014可抑制裸鼠体内的人肝细胞癌的生长[J]. 南方医科大学学报, 2021, 41(7): 1056-1061. |
| [7] | 翟东凤, 王 鸽, 李 蕾, 贾小婷, 郑国沛, 尹 江. m6A修饰调控的LDB2抑制肺腺癌细胞增殖[J]. 南方医科大学学报, 2021, 41(3): 329-335. |
| [8] | 刘 铸, 郭泽钦, 龙利丽, 张艳培, 卢钰雯, 吴德华, 董忠谊. SAC复合体相关基因TTK和MAD2L1基因在肺腺癌中过表达:基于大数据的生物信息学分析[J]. 南方医科大学学报, 2020, 40(10): 1422-1431. |
| [9] | 彭淑贤,李浔,刘琴,张颖恒,邹黎明,龚小莉,王苗淼,马晓冬. 转录组数据分析肺腺癌和肺鳞状细胞癌中基因的差异表达[J]. 南方医科大学学报, 2019, 39(06): 641-. |
| [10] | 李利,张婷婷,陈玉华,宋佳,孟瑶,刘姝,谢剑明. 转录因子SOX12在肺腺癌中的表达及其与临床预后的关系[J]. 南方医科大学学报, 2019, 39(02): 186-. |
| [11] | 何萍,顾霞,曾欣,郑咏玫,林晓东. 肺原位腺癌、微浸润腺癌及浸润性腺癌中淋巴管密度的变化及其调控因子[J]. 南方医科大学学报, 2018, 38(11): 1349-. |
| [12] | 王玉环,张淑华,穆淑坤,张柏深,马树东. 去泛素化酶USP33通过下调SLIT2/ROBO1信号通路抑制肺腺癌的侵袭和转移[J]. 南方医科大学学报, 2018, 38(08): 956-. |
| [13] | 潘莹,黄思超,王霞,龚五星,梁翠微,杜均祥,彭东旭,谢云,郑礼平,张楠,全文. NF-κB亚单位p50/p65激活促进肺腺癌H1650细胞吉非替尼耐药[J]. 南方医科大学学报, 2018, 38(05): 584-. |
| [14] | 陈帅,周永春,陈颖,陈小波,李光剑,杨加鹏,雷玉洁,赵光强,黄秋博,杨长绍,杜亚茜,黄云超. 宣威地区肺腺癌病人肺组织特异miRNAs表达谱和靶基因及其信号通路预测[J]. 南方医科大学学报, 2017, 37(02): 238-. |
| [15] | 徐小艳,刘红伟,姜黄,李川,袁淑慧,杨金花. 联合检测细胞蜡块中的napsin A和甲状腺转录因子-1有助于肺腺癌胸水的诊断[J]. 南方医科大学学报, 2015, 35(11): 1610-. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||