南方医科大学学报 ›› 2025, Vol. 45 ›› Issue (2): 213-222.doi: 10.12122/j.issn.1673-4254.2025.02.01
• • 下一篇
刘新颜1,2( ), 范琪3(), 邓明芬1,2, 许言1,2, 郭静1,2, 曹苹4,5, 周灿权1,2, 徐艳文1,2()
), 范琪3(), 邓明芬1,2, 许言1,2, 郭静1,2, 曹苹4,5, 周灿权1,2, 徐艳文1,2()
收稿日期:2024-11-06
接受日期:2024-12-06
出版日期:2025-02-20
发布日期:2025-03-03
通讯作者:
徐艳文
E-mail:liuxy6@mail.sysu.edu.cn;fanqi1058559207@126.com;xuyanwen@mail.sysu.edu.cn
作者简介:刘新颜, 博士后, 医师, E-mail: liuxy6@mail.sysu.edu.cn基金资助:
Xinyan LIU1,2(), Qi FAN3(), Mingfen DENG1,2, Yan XU1,2, Jing GUO1,2, Ping CAO4,5, Canquan ZHOU1,2, Yanwen XU1,2()
Received:2024-11-06
Accepted:2024-12-06
Online:2025-02-20
Published:2025-03-03
Contact:
Yanwen XU
E-mail:liuxy6@mail.sysu.edu.cn;fanqi1058559207@126.com;xuyanwen@mail.sysu.edu.cn
About author:First author contact:刘新颜、范 琪共同为第一作者
Supported by:摘要:
目的 评估雄激素受体(AR)的GGN重复多态性与卵巢储备及在控制性卵巢刺激(COS)中的卵巢反应的关联。 方法 在一所大学附属的体外授精胚胎移植中心进行的这项遗传关联研究中,共有361名年龄≤40岁、基础卵泡刺激素≤12 IU/L的女性接受了GnRH激动剂长方案进行COS。对AR基因中的GGN重复进行了Sanger测序分析。主要终点是窦卵泡计数(AFCs),次要终点包括刺激天数、使用的促性腺激素(Gn)总剂量、取卵总数、卵巢敏感性指数(OSI)和卵泡输出率(FORT)。 结果 AR基因第1外显子中的GGN重复长度13~24,观察到的中位重复长度为22。考虑基因型(GGN重复<22为S,GGN重复≥22为L)时,所有患者被分为3组:SS、SL和LL。广义回归分析指出,SS组的AFCs数量显著低于SL组(调整后β值1.8;95% CI:0.2-3.4;P=0.024)或与LL组比较(调整后β值1.5;95% CI:0.2-2.7;P=0.021)。SL组与LL组之间的AFCs数量没有观察到显著差异。此外,广义回归分析还表明,在调整混杂因素前后,3组之间的卵巢刺激参数差异没有统计学意义。 结论 AR基因上的GGN重复长度与AFC相关,但与中国女性的卵巢反应无关,表明AR基因的多态性可能影响卵巢储备。
刘新颜, 范琪, 邓明芬, 许言, 郭静, 曹苹, 周灿权, 徐艳文. 雄激素受体基因的GGN重复长度与接受控制性卵巢刺激的中国女性的窦卵泡计数相关[J]. 南方医科大学学报, 2025, 45(2): 213-222.
Xinyan LIU, Qi FAN, Mingfen DENG, Yan XU, Jing GUO, Ping CAO, Canquan ZHOU, Yanwen XU. GGN repeat length of the androgen receptor gene is associated with antral follicle count in Chinese women undergoing controlled ovarian stimulation[J]. Journal of Southern Medical University, 2025, 45(2): 213-222.
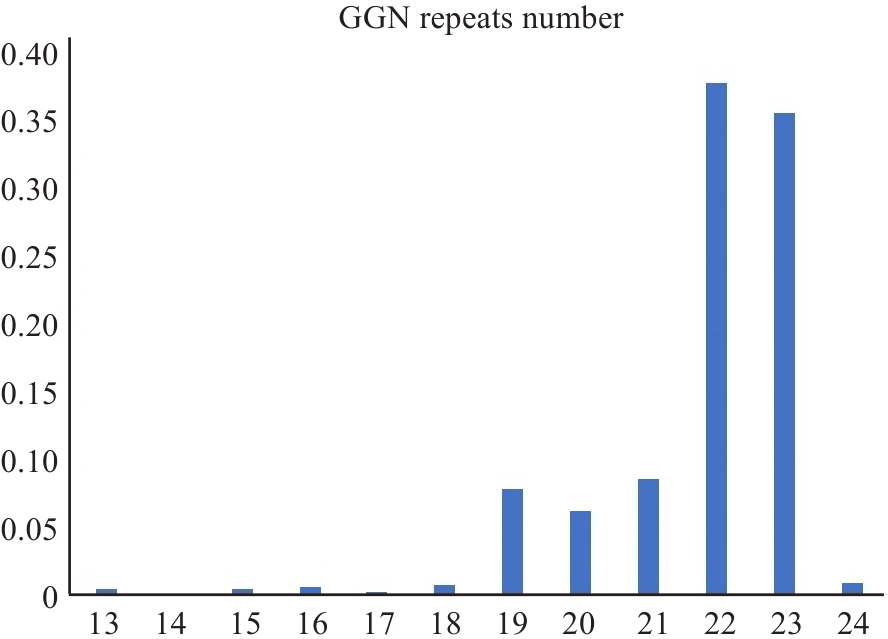
Fig.1 Distribution of GGN repeats of androgen receptor (AR) in female patients undergoing IVF treatment.
| Parameters | SS group | SL group | LL group | P value | Total |
|---|---|---|---|---|---|
| No. | 62 | 58 | 241 | 361 | |
| BMI (kg/m2) | 20.9±2.3 | 20.6±2.3 | 21.0±2.6 | 0.447 | 20.9±2.5 |
| Female age (years) | 29.8±3.8 | 30.3±3.8 | 30.1±3.7 | 0.700 | 30.1±3.8 |
| Menarche age (years) | 13.3±1.6 | 14.0±1.5 | 13.8±1.4 | 0.025 | 13.7±1.5 |
| Menstrual cycle (days) | 31.7±7.4 | 30.5±2.5 | 30.4±3.7 | 0.108 | 30.6±4.4 |
| No.of previous pregnancies* | 1.0 (0.0-4.0) | 1.0 (0.0-3.0) | 0.0 (0.0-7.0) | 0.349 | 0.0 (0.0-7.0) |
| No.of live births* | 0.0 (0.0-2.0) | 0.0 (0.0-1.0) | 0.0 (0.0-2.0) | 0.855 | 0.0 (0.0-2.0) |
| No.of spontaneous abortions* | 0.0 (0.0-2.0) | 0.0 (0.0-3.0) | 0.0 (0.0-4.0) | 0.065 | 0.0 (0.0-4.0) |
| No.of ectopic pregnancies* | 0.0 (0.0-3.0) | 0.0 (0.0-2.0) | 0.0 (0.0-4.0) | 0.797 | 0.0 (0.0-4.0) |
| Years of infertility | 3.2±2.8 | 3.5±2.6 | 3.6±2.8 | 0.738 | 3.5±2.7 |
| Education level | 0.812 | ||||
| Primary school | 0 (0.0%) | 0 (0.0%) | 4 (1.7%) | 4 (1.1%) | |
| Middle/high school | 38 (61.3%) | 38 (65.5%) | 148 (61.4%) | 224 (62.0%) | |
| University | 23 (37.1%) | 18 (31.0%) | 84 (34.9%) | 125 (34.6%) | |
| Postgraduate | 1 (1.6%) | 2 (3.4%) | 5 (2.1%) | 8 (2.2%) | |
| Types of infertility | 0.364 | ||||
| No infertility | 4 (6.5%) | 6 (10.3%) | 26 (10.8%) | 36 (10.0%) | |
| Primary infertility | 29 (46.8%) | 26 (44.8%) | 130 (53.9%) | 185 (51.2%) | |
| Secondary infertility | 29 (46.8%) | 26 (44.8%) | 85 (35.3%) | 140 (38.8%) | |
| Indicator of IVF | 0.318 | ||||
| Infertility/female factors | 11 (17.7%) | 16 (27.6%) | 34 (14.1%) | 61 (16.9%) | |
| Infertility/male factors | 19 (30.6%) | 17 (29.3%) | 78 (32.4%) | 114 (31.6%) | |
| Infertility/coupled factors | 24 (38.7%) | 17 (29.3%) | 86 (35.7%) | 127 (35.2%) | |
| Monogenic diseases | 8 (12.9%) | 8 (13.8%) | 43 (17.8%) | 59 (16.3%) | |
| Basal FSH (mIU/mL) | 5.7±1.4 | 5.5±1.4 | 5.5±1.4 | 0.745 | 5.5±1.4 |
| Basal LH (mIU/mL) | 4.2±1.9 | 3.8±1.5 | 3.9±2.0 | 0.542 | 3.9±1.9 |
| Basal E2 (pg/ml) | 36.1±15.3 | 34.5±12.2 | 38.2±14.4 | 0.154 | 37.3±14.3 |
| Testosterone (ng/mL) | 0.3±0.1 | 0.3±0.1 | 0.3±0.2 | 0.274 | 0.3±0.1 |
| AFC | 12.9±4.4 | 14.4±3.7 | 14.1±4.8 | 0.138 | 13.9±4.6 |
| GnRHa protocol | 0.164 | ||||
| 0.01 | 34 (54.8%) | 41 (70.7%) | 158 (65.6%) | 233 (64.5%) | |
| 0.01-0.05 | 28 (45.2%) | 17 (29.3%) | 83 (34.4%) | 128 (35.5%) | |
| Starting dose of Gn (IU) | 184.9±45.6 | 174.1±39.8 | 182.9±46.8 | 0.358 | 181.8±45.6 |
| Stimulation days | 10.2±1.4) | 10.1±1.6 | 10.2±1.6 | 0.963 | 10.2±1.5 |
| Total dose of Gn (IU) | 1917.8±680.2 | 1777.9±568.7 | 1890.4±692.4 | 0.453 | 1877.0±671.7 |
| No.of retrieved oocytes | 15.5±8.1 | 17.2±6.9 | 15.7±6.6 | 0.286 | 15.9±6.9 |
| OSI* | 115.9 (27.6- 662.5) | 104.7 (39.3- 510.0) | 116.7 (33.5-2925.0) | 0.317 | 115.2 (27.6-2925.0) |
| FORT | 0.6±0.2 | 0.6±0.2 | 0.6±0.2 | 0.379 | 0.6±0.2 |
| Biallelic mean | 19.3±1.4 | 21.4 (0.7) | 22.5±0.2 | <0.001 | 21.8±1.4 |
| FSHR genotypes | 0.597 | ||||
| C/C | 4 (6.5%) | 6 (10.3%) | 24 (10.0%) | 34 (9.5%) | |
| C/T | 27 (43.5%) | 20 (34.5%) | 106 (44.4%) | 153 (42.6%) | |
| T/T | 31 (50.0%) | 32 (55.2%) | 109 (45.6%) | 172 (47.9%) |
Tab.1 General clinical characteristics of 361 Chinese women undergoing IVF in groups SS, SL and LL
| Parameters | SS group | SL group | LL group | P value | Total |
|---|---|---|---|---|---|
| No. | 62 | 58 | 241 | 361 | |
| BMI (kg/m2) | 20.9±2.3 | 20.6±2.3 | 21.0±2.6 | 0.447 | 20.9±2.5 |
| Female age (years) | 29.8±3.8 | 30.3±3.8 | 30.1±3.7 | 0.700 | 30.1±3.8 |
| Menarche age (years) | 13.3±1.6 | 14.0±1.5 | 13.8±1.4 | 0.025 | 13.7±1.5 |
| Menstrual cycle (days) | 31.7±7.4 | 30.5±2.5 | 30.4±3.7 | 0.108 | 30.6±4.4 |
| No.of previous pregnancies* | 1.0 (0.0-4.0) | 1.0 (0.0-3.0) | 0.0 (0.0-7.0) | 0.349 | 0.0 (0.0-7.0) |
| No.of live births* | 0.0 (0.0-2.0) | 0.0 (0.0-1.0) | 0.0 (0.0-2.0) | 0.855 | 0.0 (0.0-2.0) |
| No.of spontaneous abortions* | 0.0 (0.0-2.0) | 0.0 (0.0-3.0) | 0.0 (0.0-4.0) | 0.065 | 0.0 (0.0-4.0) |
| No.of ectopic pregnancies* | 0.0 (0.0-3.0) | 0.0 (0.0-2.0) | 0.0 (0.0-4.0) | 0.797 | 0.0 (0.0-4.0) |
| Years of infertility | 3.2±2.8 | 3.5±2.6 | 3.6±2.8 | 0.738 | 3.5±2.7 |
| Education level | 0.812 | ||||
| Primary school | 0 (0.0%) | 0 (0.0%) | 4 (1.7%) | 4 (1.1%) | |
| Middle/high school | 38 (61.3%) | 38 (65.5%) | 148 (61.4%) | 224 (62.0%) | |
| University | 23 (37.1%) | 18 (31.0%) | 84 (34.9%) | 125 (34.6%) | |
| Postgraduate | 1 (1.6%) | 2 (3.4%) | 5 (2.1%) | 8 (2.2%) | |
| Types of infertility | 0.364 | ||||
| No infertility | 4 (6.5%) | 6 (10.3%) | 26 (10.8%) | 36 (10.0%) | |
| Primary infertility | 29 (46.8%) | 26 (44.8%) | 130 (53.9%) | 185 (51.2%) | |
| Secondary infertility | 29 (46.8%) | 26 (44.8%) | 85 (35.3%) | 140 (38.8%) | |
| Indicator of IVF | 0.318 | ||||
| Infertility/female factors | 11 (17.7%) | 16 (27.6%) | 34 (14.1%) | 61 (16.9%) | |
| Infertility/male factors | 19 (30.6%) | 17 (29.3%) | 78 (32.4%) | 114 (31.6%) | |
| Infertility/coupled factors | 24 (38.7%) | 17 (29.3%) | 86 (35.7%) | 127 (35.2%) | |
| Monogenic diseases | 8 (12.9%) | 8 (13.8%) | 43 (17.8%) | 59 (16.3%) | |
| Basal FSH (mIU/mL) | 5.7±1.4 | 5.5±1.4 | 5.5±1.4 | 0.745 | 5.5±1.4 |
| Basal LH (mIU/mL) | 4.2±1.9 | 3.8±1.5 | 3.9±2.0 | 0.542 | 3.9±1.9 |
| Basal E2 (pg/ml) | 36.1±15.3 | 34.5±12.2 | 38.2±14.4 | 0.154 | 37.3±14.3 |
| Testosterone (ng/mL) | 0.3±0.1 | 0.3±0.1 | 0.3±0.2 | 0.274 | 0.3±0.1 |
| AFC | 12.9±4.4 | 14.4±3.7 | 14.1±4.8 | 0.138 | 13.9±4.6 |
| GnRHa protocol | 0.164 | ||||
| 0.01 | 34 (54.8%) | 41 (70.7%) | 158 (65.6%) | 233 (64.5%) | |
| 0.01-0.05 | 28 (45.2%) | 17 (29.3%) | 83 (34.4%) | 128 (35.5%) | |
| Starting dose of Gn (IU) | 184.9±45.6 | 174.1±39.8 | 182.9±46.8 | 0.358 | 181.8±45.6 |
| Stimulation days | 10.2±1.4) | 10.1±1.6 | 10.2±1.6 | 0.963 | 10.2±1.5 |
| Total dose of Gn (IU) | 1917.8±680.2 | 1777.9±568.7 | 1890.4±692.4 | 0.453 | 1877.0±671.7 |
| No.of retrieved oocytes | 15.5±8.1 | 17.2±6.9 | 15.7±6.6 | 0.286 | 15.9±6.9 |
| OSI* | 115.9 (27.6- 662.5) | 104.7 (39.3- 510.0) | 116.7 (33.5-2925.0) | 0.317 | 115.2 (27.6-2925.0) |
| FORT | 0.6±0.2 | 0.6±0.2 | 0.6±0.2 | 0.379 | 0.6±0.2 |
| Biallelic mean | 19.3±1.4 | 21.4 (0.7) | 22.5±0.2 | <0.001 | 21.8±1.4 |
| FSHR genotypes | 0.597 | ||||
| C/C | 4 (6.5%) | 6 (10.3%) | 24 (10.0%) | 34 (9.5%) | |
| C/T | 27 (43.5%) | 20 (34.5%) | 106 (44.4%) | 153 (42.6%) | |
| T/T | 31 (50.0%) | 32 (55.2%) | 109 (45.6%) | 172 (47.9%) |
| Exposure | Non-adjusted β (95% Cl) | P | Model aβ (95% Cl) | P | Model bβ (95%Cl) | P |
|---|---|---|---|---|---|---|
| GGN groups | ||||||
| SS | 0 | 0 | 0 | |||
| SL | 1.5 (-0.1, 3.2) | 0.074 | 1.8 (0.2, 3.4) | 0.024 | 1.6 (0.0, 3.1) | 0.047 |
| LL | 1.2 (-0.1, 2.5) | 0.073 | 1.5 (0.2, 2.7) | 0.021 | 1.4 (0.2, 2.6) | 0.027 |
Tab.2 Number of AFCs among groups SS, SL and LL
| Exposure | Non-adjusted β (95% Cl) | P | Model aβ (95% Cl) | P | Model bβ (95%Cl) | P |
|---|---|---|---|---|---|---|
| GGN groups | ||||||
| SS | 0 | 0 | 0 | |||
| SL | 1.5 (-0.1, 3.2) | 0.074 | 1.8 (0.2, 3.4) | 0.024 | 1.6 (0.0, 3.1) | 0.047 |
| LL | 1.2 (-0.1, 2.5) | 0.073 | 1.5 (0.2, 2.7) | 0.021 | 1.4 (0.2, 2.6) | 0.027 |
| Secondary outcomes | Non-adjusted β (95% Cl) | P | Model aβ (95% Cl) | P |
|---|---|---|---|---|
| Stimulation days | ||||
| SS | 0 | 0 | ||
| SL | -0.1 (-0.6, 0.5) | 0.841 | -0.0 (-0.6, 0.6) | 0.996 |
| LL | 0.0 (-0.4, 0.4) | 0.981 | 0.0 (-0.4, 0.5) | 0.876 |
| Total dose of Gn | ||||
| SS | 0 | 0 | ||
| SL | -139.9 (-380.5, 100.8) | 0.255 | -153.7 (-363.0, 55.5) | 0.151 |
| LL | -27.3 (-214.9, 160.3) | 0.775 | -61.3 (-224.6, 101.9) | 0.462 |
| No.of retrieved oocytes | ||||
| SS | 0 | 0 | ||
| SL | 1.7 (-0.8, 4.2) | 0.178 | 1.7 (-0.9, 4.2) | 0.199 |
| SL | 0.2 (-1.7, 2.1) | 0.852 | 0.1 (-1.9, 2.0) | 0.944 |
| OSI | ||||
| SS | 0 | 0 | ||
| SL | -34.4 (-109.7, 40.9) | 0.371 | -25.2 (-97.6, 47.3) | 0.496 |
| LL | 12.1 (-46.5, 70.8) | 0.685 | 8.9 (-47.7, 65.4) | 0.759 |
| FORT | ||||
| SS | 0 | 0 | ||
| SL | -0.0 (-0.1, 0.1) | 0.593 | -0.0 (-0.1, 0.0) | 0.362 |
| LL | -0.0 (-0.1, 0.0) | 0.180 | -0.0 (-0.1, 0.0) | 0.145 |
Tab.3 Ovarian response parameters among groups SS, SL and LL
| Secondary outcomes | Non-adjusted β (95% Cl) | P | Model aβ (95% Cl) | P |
|---|---|---|---|---|
| Stimulation days | ||||
| SS | 0 | 0 | ||
| SL | -0.1 (-0.6, 0.5) | 0.841 | -0.0 (-0.6, 0.6) | 0.996 |
| LL | 0.0 (-0.4, 0.4) | 0.981 | 0.0 (-0.4, 0.5) | 0.876 |
| Total dose of Gn | ||||
| SS | 0 | 0 | ||
| SL | -139.9 (-380.5, 100.8) | 0.255 | -153.7 (-363.0, 55.5) | 0.151 |
| LL | -27.3 (-214.9, 160.3) | 0.775 | -61.3 (-224.6, 101.9) | 0.462 |
| No.of retrieved oocytes | ||||
| SS | 0 | 0 | ||
| SL | 1.7 (-0.8, 4.2) | 0.178 | 1.7 (-0.9, 4.2) | 0.199 |
| SL | 0.2 (-1.7, 2.1) | 0.852 | 0.1 (-1.9, 2.0) | 0.944 |
| OSI | ||||
| SS | 0 | 0 | ||
| SL | -34.4 (-109.7, 40.9) | 0.371 | -25.2 (-97.6, 47.3) | 0.496 |
| LL | 12.1 (-46.5, 70.8) | 0.685 | 8.9 (-47.7, 65.4) | 0.759 |
| FORT | ||||
| SS | 0 | 0 | ||
| SL | -0.0 (-0.1, 0.1) | 0.593 | -0.0 (-0.1, 0.0) | 0.362 |
| LL | -0.0 (-0.1, 0.0) | 0.180 | -0.0 (-0.1, 0.0) | 0.145 |
| 1 | Walters KA, Allan CM, Handelsman DJ. Androgen actions and the ovary[J]. Biol Reprod, 2008, 78(3): 380-9. DOI: 10.1095/biolreprod.107.064089 |
| 2 | Suzuki T, Sasano H, Kimura N, et al. Immunohistochemical distribution of progesterone, androgen and oestrogen receptors in the human ovary during the menstrual cycle: relationship to expression of steroidogenic enzymes[J]. Hum Reprod, 1994, 9(9): 1589-95. DOI: 10.1093/oxfordjournals.humrep.a138757 |
| 3 | Gleicher N, Weghofer A, Barad DH. The role of androgens in follicle maturation and ovulation induction: friend or foe of infertility treatment[J]? Reprod Biol Endocrinol, 2011, 9: 116. DOI: 10.1186/1477-7827-9-116 |
| 4 | Li M, Schatten H, Sun QY. Androgen receptor's destiny in mammalian oocytes: a new hypothesis[J]. Mol Hum Reprod, 2009, 15(3): 149-54. DOI: 10.1093/molehr/gap006 |
| 5 | Yeh S, Tsai MY, Xu QQ, et al. Generation and characterization of androgen receptor knockout (ARKO) mice: an in vivo model for the study of androgen functions in selective tissues[J]. Proc Natl Acad Sci USA, 2002, 99(21): 13498-503. DOI: 10.1073/pnas.212474399 |
| 6 | Hu YC, Wang PH, Yeh S, et al. Subfertility and defective folliculogenesis in female mice lacking androgen receptor[J]. Proc Natl Acad Sci U S A, 2004, 101(31): 11209-14. DOI: 10.1073/pnas.0404372101 |
| 7 | Shiina H, Matsumoto T, Sato T, et al. Premature ovarian failure in androgen receptor-deficient mice[J]. Proc Natl Acad Sci USA, 2006, 103(1): 224-9. DOI: 10.1073/pnas.0506736102 |
| 8 | Walters KA, Allan CM, Jimenez M, et al. Female mice haploinsufficient for an inactivated androgen receptor (AR) exhibit age-dependent defects that resemble the AR null phenotype of dysfunctional late follicle development, ovulation, and fertility[J]. Endocrinology, 2007, 148(8): 3674-84. DOI: 10.1210/en.2007-0248 |
| 9 | Kittles RA, Young D, Weinrich S, et al. Extent of linkage disequilibrium between the androgen receptor gene CAG and GGC repeats in human populations: implications for prostate cancer risk[J]. Hum Genet, 2001, 109(3): 253-61. DOI: 10.1007/s004390100576 |
| 10 | Gilbert SM, Benson MC, McKiernan JM. Linkage disequilibrium between the androgen receptor gene CAG and GGC repeats in the African-American population[J]. Curr Urol Rep, 2002, 3(3): 189-93. DOI: 10.1007/s11934-002-0063-y |
| 11 | Irvine RA, Yu MC, Ross RK, et al. The CAG and GGC microsatellites of the androgen receptor gene are in linkage disequilibrium in men with prostate cancer[J]. Cancer Res, 1995, 55(9): 1937-40. |
| 12 | Henningsson S, Jonsson L, Ljunggren E, et al. Possible association between the androgen receptor gene and autism spectrum disorder[J]. Psychoneuroendocrinology, 2009, 34(5): 752-61. DOI: 10.1016/j.psyneuen.2008.12.007 |
| 13 | Lumbroso R, Beitel LK, Vasiliou DM, et al. Codon-usage variants in the polymorphic (GGN)n trinucleotide repeat of the human androgen receptor gene[J]. Hum Genet, 1997, 101(1): 43-6. DOI: 10.1007/s004390050583 |
| 14 | Albertelli MA, Scheller A, Brogley M, et al. Replacing the mouse androgen receptor with human alleles demonstrates glutamine tract length-dependent effects on physiology and tumorigenesis in mice[J]. Mol Endocrinol, 2006, 20(6): 1248-60. DOI: 10.1210/me.2006-0021 |
| 15 | Davis-Dao CA, Tuazon ED, Sokol RZ, et al. Male infertility and variation in CAG repeat length in the androgen receptor gene: a meta-analysis[J]. J Clin Endocrinol Metab, 2007, 92(11): 4319-26. DOI: 10.1210/jc.2007-1110 |
| 16 | Qin ZQ, Li X, Han P, et al. Association between polymorphic CAG repeat lengths in the androgen receptor gene and susceptibility to prostate cancer: a systematic review and meta-analysis[J]. Medicine, 2017, 96(25): e7258. DOI: 10.1097/md.0000000000007258 |
| 17 | Gao T, Marcelli M, McPhaul MJ. Transcriptional activation and transient expression of the human androgen receptor[J]. J Steroid Biochem Mol Biol, 1996, 59(1): 9-20. DOI: 10.1016/s0960-0760(96)00097-0 |
| 18 | Grigorova M, Punab M, Kahre T, et al. The number of CAG and GGN triplet repeats in the Androgen Receptor gene exert combinatorial effect on hormonal and sperm parameters in young men[J]. Andrology, 2017, 5(3): 495-504. DOI: 10.1111/andr.12344 |
| 19 | Moghadam M, Khatami SR, Galehdari H. Association of androgen receptor GGN repeat length polymorphism and male infertility in Khuzestan, Iran[J]. Iran J Reprod Med, 2015, 13(5): 305-10. |
| 20 | Han TT, Ran J, Ding XP, et al. Cytogenetic and molecular analysis of infertile Chinese men: karyotypic abnormalities, Y-chromosome microdeletions, and CAG and GGN repeat polymorphisms in the androgen receptor gene[J]. Genet Mol Res, 2013, 12(3): 2215-26. DOI: 10.4238/2013.july.8.3 |
| 21 | Zhang C, Dang J, Xu H, et al. Associations between androgen receptor CAG & GGN repeat polymorphism & recurrent spontaneous abortions in Chinese women[J]. Indian J Med Res, 2014, 139(5): 730-6. |
| 22 | Suter NM, Malone KE, Daling JR, et al. Androgen receptor (CAG)n and (GGC)n polymorphisms and breast cancer risk in a population-based case-control study of young women[J]. Cancer Epidemiol Biomarkers Prev, 2003, 12(2): 127-35. |
| 23 | Lledó B, Llácer J, Turienzo A, et al. Androgen receptor CAG repeat length is associated with ovarian reserve but not with ovarian response[J]. Reprod Biomed Online, 2014, 29(4): 509-15. DOI: 10.1016/j.rbmo.2014.06.012 |
| 24 | Yuan C, Gao C, Qian Y, et al. Polymorphism of CAG and GGN repeats of androgen receptor gene in women with polycystic ovary syndrome[J]. Reprod Biomed Online, 2015, 31(6): 790-8. DOI: 10.1016/j.rbmo.2015.09.007 |
| 25 | Panda B, Rao L, Tosh D, et al. Germline study of AR gene of Indian women with ovarian failure[J]. Gynecol Endocrinol, 2011, 27(8): 572-8. DOI: 10.3109/09513590.2010.507282 |
| 26 | Broekmans FJ, de Ziegler D, Howles CM, et al. The antral follicle count: practical recommendations for better standardization[J]. Fertil Steril, 2010, 94(3): 1044-51. DOI: 10.1016/j.fertnstert.2009.04.040 |
| 27 | Biasoni V, Patriarca A, Dalmasso P, et al. Ovarian sensitivity index is strongly related to circulating AMH and may be used to predict ovarian response to exogenous gonadotropins in IVF[J]. Reprod Biol Endocrinol, 2011, 9: 112. DOI: 10.1186/1477-7827-9-112 |
| 28 | Gallot V, Berwanger da Silva AL, Genro V, et al. Antral follicle responsiveness to follicle-stimulating hormone administration assessed by the Follicular Output RaTe (FORT) may predict in vitro fertilization-embryo transfer outcome[J]. Hum Reprod, 2012, 27(4): 1066-72. DOI: 10.1093/humrep/der479 |
| 29 | Dewailly D, Robin G, Peigne M, et al. Interactions between androgens, FSH, anti-Müllerian hormone and estradiol during folliculogenesis in the human normal and polycystic ovary[J]. Hum Reprod Update, 2016, 22(6): 709-24. DOI: 10.1093/humupd/dmw027 |
| 30 | Yang JL, Zhang CP, Li L, et al. Testosterone induces redistribution of forkhead box-3a and down-regulation of growth and differentiation factor 9 messenger ribonucleic acid expression at early stage of mouse folliculogenesis[J]. Endocrinology, 2010, 151(2): 774-82. DOI: 10.1210/en.2009-0751 |
| 31 | Pan JX, Zhang JY, Ke ZH, et al. Androgens as double-edged swords: induction and suppression of follicular development[J]. Hormones, 2015, 14(2): 190-200. DOI: 10.14310/horm.2002.1580 |
| 32 | Fábregues F, Peñarrubia J, Creus M, et al. Transdermal testosterone may improve ovarian response to gonadotrophins in low-responder IVF patients: a randomized, clinical trial[J]. Hum Reprod, 2009, 24(2): 349-59. DOI: 10.1093/humrep/den428 |
| 33 | Adachi M, Takayanagi R, Tomura A, et al. Androgen-insensitivity syndrome as a possible coactivator disease[J]. N Engl J Med, 2000, 343(12): 856-62. DOI: 10.1056/nejm200009213431205 |
| 34 | Holte J, Brodin T, Berglund L, et al. Antral follicle counts are strongly associated with live-birth rates after assisted reproduction, with superior treatment outcome in women with polycystic ovaries[J]. Fertil Steril, 2011, 96(3): 594-9. DOI: 10.1016/j.fertnstert.2011.06.071 |
| 35 | Moon KY, Kim H, Lee JY, et al. Nomogram to predict the number of oocytes retrieved in controlled ovarian stimulation[J]. Clin Exp Reprod Med, 2016, 43(2): 112-8. DOI: 10.5653/cerm.2016.43.2.112 |
| 36 | Lavery DN, McEwan IJ. Functional characterization of the native NH2-terminal transactivation domain of the human androgen receptor: binding kinetics for interactions with TFIIF and SRC-1a[J]. Biochemistry, 2008, 47(11): 3352-9. DOI: 10.1021/bi702220p |
| 37 | McEwan IJ. Androgen receptor modulators: a marriage of chemistry and biology[J]. Future Med Chem, 2013, 5(10): 1109-20. DOI: 10.4155/fmc.13.69 |
| 38 | Burris TP, Solt LA, Wang YJ, et al. Nuclear receptors and their selective pharmacologic modulators[J]. Pharmacol Rev, 2013, 65(2): 710-78. DOI: 10.1124/pr.112.006833 |
| 39 | Ahmad AK, Kao CN, Quinn M, et al. Differential rate in decline in ovarian reserve markers in women with polycystic ovary syndrome compared with control subjects: results of a longitudinal study[J]. Fertil Steril, 2018, 109(3): 526-31. DOI: 10.1016/j.fertnstert.2017.11.012 |
| 40 | Jayaprakasan K, Campbell B, Hopkisson J, et al. A prospective, comparative analysis of anti-Müllerian hormone, inhibin-B, and three-dimensional ultrasound determinants of ovarian reserve in the prediction of poor response to controlled ovarian stimulation[J]. Fertil Steril, 2010, 93(3): 855-64. DOI: 10.1016/j.fertnstert.2008.10.042 |
| 41 | Aruna M, Dasgupta S, Sirisha PV, et al. Role of androgen receptor CAG repeat polymorphism and X-inactivation in the manifestation of recurrent spontaneous abortions in Indian women[J]. PLoS One, 2011, 6(3): e17718. DOI: 10.1371/journal.pone.0017718 |
| 42 | Zito A, Davies MN, Tsai PC, et al. Heritability of skewed X-inactivation in female twins is tissue-specific and associated with age[J]. Nat Commun, 2019, 10(1): 5339. DOI: 10.1038/s41467-019-13340-w |
| 43 | Tukiainen T, Villani AC, Yen A, et al. Landscape of X chromosome inactivation across human tissues[J]. Nature, 2017, 550(7675): 244-8. DOI: 10.1038/nature24265 |
| 44 | Godler DE, Inaba Y, Schwartz CE, et al. Detection of skewed X-chromosome inactivation in Fragile X syndrome and X chromosome aneuploidy using quantitative melt analysis[J]. Expert Rev Mol Med, 2015, 17: e13. DOI: 10.1017/erm.2015.11 |
| [1] | 常馨月, 姚宁宁, 赵燕, 王银凤, 王岸聪, 张慧辉, 张静. 外源性药物扳机可改善卵巢功能减退患者自然周期体外受精/卵胞浆内单精子注射助孕的结局:一项倾向性评分匹配及Logistic回归分析[J]. 南方医科大学学报, 2025, 45(7): 1519-1526. |
| [2] | 吴晓敏, 陈映雪, 周星宇, 张 俊, 黎 莹, 李 欣, 张笑菲, 陈士岭. 卵泡发育中晚期添加HMG可改善妊娠结局:基于682例高龄卵巢储备减退患者[J]. 南方医科大学学报, 2021, 41(3): 412-417. |
| [3] | 邓煜麟,郭凯,曾颖科,吴凯辉,唐晨,郑少波. 雄激素受体对IgG蛋白表达及前列腺癌细胞增殖和迁移的影响[J]. 南方医科大学学报, 2017, 37(03): 388-. |
| [4] | 王 楠,陈 薪,叶德盛,许丽娟,田小龙,陶 婷,陈士岭. 恶性肿瘤术后合并不孕症患者经体外受精-胚胎移植治疗获妊娠3例报道并文献复习[J]. 南方医科大学学报, 2015, 35(06): 838-. |
| [5] | 彭萍,马春玲,叶长烂,万淑梅,张艳玲,滕伟. 胎儿生长受限与成年后卵巢储备功能的关系[J]. 南方医科大学学报, 2014, 34(08): 1217-. |
| [6] | 何于夏,夏容,陈薪,叶德盛,唐妍,黎璞,牛静,陈士岭. 在体外受精-胚胎移植中应用多项卵巢储备功能评估指标预测卵巢反应性[J]. 南方医科大学学报, 2013, 33(02): 216-. |
| [7] | 陈玢屾,徐亚文,徐啊白,刘春晓,郑少波,李虎林,许凯. 多西他赛对雄激素依赖型及非依赖亚型前列腺癌细胞中C-jun与雄激素受体相互作用的影响[J]. 南方医科大学学报, 2012, 32(10): 1461-. |
| [8] | 陈士岭,夏容,陈薪,罗燕群,王乐乐,吴雅琴,施晓鋆,郑海燕. 基础窦状卵泡数结合年龄用于评估卵巢储备及预测卵巢低反应和体外受精临床结局[J]. 南方医科大学学报, 2011, 31(04): 572-. |
| [9] | 邓凡 王春霞 许万福 冯丽 柯志勇 Wang Q. Jane 邹志鹏. PKD3上调前列腺癌细胞中PSA表达及机制[J]. 南方医科大学学报, 2010, 30(08): 1779-1782. |
| [10] | 贾彬; 汤泓; 黎玮; 蔡文清;. 表皮生长因子对小鼠前列腺细胞雌雄激素受体表达的影响[J]. 南方医科大学学报, 2006, 26(10): 1473-1475. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||